Cicely G. Erskine
Title: Sex at choice
Author: Cicely Grace Erskine
Contributor: James Monteith Erskine
Release date: April 20, 2026 [eBook #78509]
Language: English
Original publication: New York: G. P. Putnam's Sons, 1925
Other information and formats: www.gutenberg.org/ebooks/78509
Credits: Tim Lindell and the Online Distributed Proofreading Team at https://www.pgdp.net (This file was produced from images generously made available by The Internet Archive)
[i]
Sex at Choice
[ii]
Cicely G. Erskine
[iii]
Sex at Choice
By
Mrs. Monteith Erskine
With an Introduction by
James Monteith Erskine
M.P. for the St. George’s Division of Westminster
G. P. Putnam’s Sons
New York & London
The Knickerbocker Press
1925
[iv]
Copyright, 1925
by
Cicely Erskine
Made in the United States of America
[v]
This book, written by a woman for women, is the result of twenty-five years’ continuous study of the causes of Sex-determination and of the most feasible method of controlling it. It represents also the work of a life-time devoted to investigation into every symptom or indication, however minute or apparently insignificant, manifested in the pregnancy of male offspring as distinct from that of female.
This research, mainly practical and clinical, was undertaken as a result of the close attention which, for some years, I had devoted to all matters connected with the health of young girls.
At an early age I came to realise the fundamental truth of the alternate action of “sides.” I use this word advisedly, because in those days [vi]I knew no other. It goes without saying that this fact was brought to my notice solely by the physical disabilities from which many girls suffer, and by the nature of the treatment which brought them relief. But, over and above this, the recognition of this truth proved, in my case, to be the key to the ultimate conclusions upon which my whole theory is based.
The study of anatomy and physiology attracted me so deeply, whilst I was yet a schoolgirl at Geneva, that it led me to further pursuit along the lines of medical enquiry. It was about this time that, by the merest chance, certain works expounding theories on sex-causation of various biologists in France and Germany came under my notice, and these I read and studied with the keenest interest.
Here it may be well to answer the constantly repeated question, “What on earth possessed you, at such an early age, to take up a subject of a nature so peculiar or, at any rate, controversial?” It must be remembered that, in the evolution of a certain train of thought, [vii]the mind is very apt to be affected by an exceptional combination of circumstances. In my own case a keen sense of the wrong which I had suffered from the start, by being born a girl where a boy was desired, had led me to vague doubts and questionings in early childhood. All this, undoubtedly, helped to sow within me the seeds of a bitter dissatisfaction with prevailing conditions. I despised the slipshod methods of biological ignorance, and justified the saying, the truth of which has so often been proved before, that “All striving towards betterment is the fruit of discontent.”
The helplessness of women in respect of any power to determine the sex of their offspring I regarded as a gross injustice and as a palpable reflection on the progress of science; not for one moment did I regard it as really due to the haphazard working of Dame Nature in her least kindly moods.
Then it was that the idea filtered slowly through my brain that it might well be a woman who alone could solve the problem. Who [viii]but a woman could have the insight, born of personal experience, the patience, produced by the physical disability of her sex, the opportunity, offered by the sympathy of her fellows, or the will, created by a burning desire to help womankind, to undertake the task of unravelling the mystery?
And so I set to work to fathom the sex-theories hitherto advanced. Most of them I speedily discarded as entirely futile and incompatible with the rôle of woman as the sole determining factor of the sexes. For I realised that even as ten lunar months are needed for the formation and perfection of the child before it is born, so also the mathematical relation of twenty-eight days or one lunar month must be applied to the periods of fertilisation in the human species. Hence, in the scientific use of these twenty-eight days must lie the predominant part of the secret of pre-determination. It was at this point that the old question “Before or After?” became a matter of very special interest and a vital object of study.
[ix]
Among competing theories there were, however, several which appeared to present material for speculation of some practical value and seemed worth testing in the light of my own observations. The results of such tests were methodically compiled in statistical form, having regard to the marked inclination of certain parents to procreate offspring of one or the other sex only. Examples were selected and added to, hundred by hundred, culled from many countries, and they represented in a marked degree distinct conditions appearing in the pregnancies of women according to the sex of the children they happened to bear.
The alternatives in connection with the time-honoured theory of “Lateral Decubitus,” which means the use of position to right or left as an assistance to sex-determination, were duly explored. And it must be borne in mind, as regards the belief of the right side being male and the left female, that this seems to have been widely accepted before any definite conclusions as to sex-theory were ever mooted. [x]The words of the first Chapter of Genesis “Male and Female created He them,” appeared to have been applied to the right or left sides of woman ever since the days of Hippocrates. The evidence of tradition, at any rate, could be cited overwhelmingly in support of it.
Again the modern suggestion that “each organ works in shifts,” was another principle of equal significance, which impressed itself upon me in the early stages of my inquiries, and I soon came to some comprehension of the alternate working of the ovaries.
During this period of my life I can say that no single instance of future maternity, still less of imminent motherhood, was discussed in my hearing, in respect to the progress and result of which I did not collect data and information. Perhaps it was owing to my keen interest in the physical sufferings of women, and my exceptional devotion to the subject of the upbringing of infants, that I so easily gained the confidence of every mother I met. The intimate details then disclosed, in [xi]exchange for the genuine sympathy I evinced in their maladies, real or even imaginary, proved of immeasurable value in my researches. Every detail of gestation and parturition was faithfully recorded, and this collection of notes became of incalculable value in helping me to establish my conclusion.
I must not forget the debt I owe to certain medical friends, who, aware of my desire for knowledge, and thinking I wished to become, in course of time, a physician, were kind enough to help me to acquire such scientific learning as might prove useful to my career.
Then came marriage with its attendant responsibilities. Five children were born to me alive and healthy, and they proved to be, as I desired, one girl and four boys. I suffered no lack of varied experiences, and took every advantage offered by all those accidental occurrences and disabilities that few mothers of large families entirely escape. Every mishap, every trouble, became a step in the progress of my ever-widening investigation.
[xii]
Eventually, as the result of much valuable and varied experience, I obtained a record of personal symptoms which might fairly claim to be unique. To these I added the data collected from other similar cases I had observed, my opportunities of observation having rapidly increased as I displayed, with greater assurance, the zeal that possessed me for more, and yet more, clinical experience and evidence. I think that an exceptionally intuitive and even hypersensitive temperament, combined with a capacity for patient plodding, helped me, as did also my complete freedom from all the restraint of a hide-bound tradition, which in so many cases hampers the outlook of the orthodox medical student.
It was in July, 1908, that, acting on the kindly advice of an eminent gynæcologist, I deposited with my bankers the actual formula which I had tested for the practical application of my theory, and which I had, in many cases, used to my own complete satisfaction. I took this step in order that I might prevent [xiii]any doubt arising in later years over my claim of priority. But even then my formula was not as complete as I wished it to be. Since that time I have made good progress in many directions, and more especially in the problem of safe-guarding from female issue those women who are not entirely normal, in that the action of their left ovary does not correspond with the laws that hold for the absolutely healthy woman.
Since 1909, people from many countries have consulted me about their future offspring. Letters of acknowledgment and testimony to the efficacy of my plans have flowed in from every part of the world.
It has been objected by some that parts of my theory have the flavour of an “old wives’ tale.” There is, indeed, some truth in this. But I see nothing to be ashamed of in the fact that my experience has tallied with that of scores of observant old ladies in past generations. Our grandmothers lived so simply and so close to nature that they were admirably [xiv]equipped for observation. They made full use of the opportunities offered them by the large families that they bore and reared, unaided and unaffected by the artificialities of civilisation. Then, as the years rolled by, the wisdom they had collected was passed on from mother to daughter, and to daughter-in-law, to survive triumphantly the passing ridicule hurled at them by cynics of all times.
But if there is in these fables much that deserves our consideration, there is also much that is entirely worthless, based on mere superstition or foolish surmise. Among these the Diet theory, which boldly proposed to change the sex of the infant in embryo by administering special food to the mother, is conspicuous. Other suggestions there were which traced the sex of the offspring to the relative ages of husband and wife, their temperaments, or a comparison between the more robust health of one parent and the weaker constitution of the other; and of all these we may safely say that where six examples can be produced to [xv]prove any one of them, half-a-dozen are forthcoming to establish the contrary.
On the other hand, the hundreds of documents I have received, and the mass of evidence, direct and indirect, I have collected, go far to place the theory of the action of the ovaries beyond question, while the very prevalent belief in Lateral Decubitus strengthened my hand considerably in making the deductions necessary to elaborate and consolidate my own theory.
And here I must touch on the far more important question of the exact periods within the 28 days of the “Lunar month” which are of such vital importance to sex-determination. I have received a vast amount of testimony on this score, and in every case it has supported the contention I have so long advanced. The conception of males would offer, to many biologists, no difficult problem. There has been little dispute as regards the times when the male ovum is capable of fertilisation. But the stumbling block has always been the question [xvi]of girl-conception, and this I maintain, is due solely to ignorance of the workings of the left ovary, as distinct from that of the right.
Some writers assert that “after the 15th day of the lunar month no conception can take place.” Then how can one account for the thousands of infants conceived in the week preceding the period—a fact so easily proved, beyond all doubt? Others again suggest the use of “early fertilisation for females” and “late fertilisation for males,” on the principle used by many breeders for cows in their first or second “heat.”
But this is precisely where I am at variance with all preconceived ideas and hitherto more or less accepted suggestions, for I maintain that woman stands apart and is unique in the exercise of her creative functions.
In 1907 A. Pohlmann published a treatise on “the heredity of the upright position and some of its disadvantages.” From the woman’s point of view one of the greatest of these is perhaps the freak working of the left [xvii]ovary. It is frequently argued that if one sex-law holds good for all other mammiferous animals, why not for woman also?
The answer is fourfold, and can hardly escape the notice of those who stop to consider the actual nature of woman’s habits and to compare them with those of the quadrupeds:
1. Woman enjoys the “disadvantages” of the upright position, which throws infinitely more strain on the genital organs than there would be, were she to live on all fours.
2. No analogy exists between her menstrual characteristics and those of animals, her courses differing in substance and quantity from the corresponding condition in quadrupeds.
3. Woman alone refrains naturally from all sexual co-habitation at these times.
4. Ovulation and menstruation, though interdependent to a great degree, are in no way simultaneous as with animals; on the contrary, the further removed from the actual [xviii]courses the healthier the impregnation of the ovum.
The flagrant contradictions prevailing among the “Before and After” theorists have also done their share for many years in baffling those biologists who have pursued their enquiry into the domain of pre-determination. It was the solution of this problem that I long ago made my goal, and it is upon this rock that my whole theory is built.
Another point which gave me much trouble, was the apparent anomaly of children of one or the other sex being born when either or both ovaries had been removed. This seemingly unaccountable event was widely discussed some generations ago, but insufficient evidence was produced to convince sceptics who contented themselves with a superficial survey of the problem. Now, for my own satisfaction, and that of all inquirers, I can safely vouch for the fact that, after the removal of one ovary, the ensuing children are, in all but the [xix]most exceptional cases, of the sex belonging to the remaining organ. And for every two or three cases supporting such an exception I have collected a hundred proving the rule.
Regarding the question of the increased activity of the one ovary following the disability of the other, I may state that the study of this momentous truth, and the collection of corroborative data, has been not the least interesting part of my work. Perhaps I may be permitted to point out that no doctor could possibly have had such opportunities as I have had of examining, from the one standpoint of sex-determination, hundreds and thousands of varied cases. Among these are women who have:
1. Been childless.
2. Had female issue only.
3. Had male issue only.
4. Had twins of the same sex.
5. Had twins of mixed sex.
Not a day passes without some fresh corroboration of the theory I here maintain reaching [xx]me. Had I ever, among all this mass of confirmation, received a single atom of conflicting evidence, it might have made me doubtful of myself. But on the contrary, the letters which for many years past, I have been continually receiving, while they often gave me food for thought, have inspired my work and spurred me on to fresh efforts.
I have realised that the limitation of families is largely the result of powerlessness to choose the sex of the offspring. The doubtful methods used in “Birth Control” have no place in my scheme, and I refuse to believe that Nature intended married life to be made unnatural by so-called “preventives.” Is it wholly absurd to believe that self-restraint in men is not unattainable, and that the exercise of self-control in conjugal life is altogether unnatural?
But, because I know so much of women’s lives, and believe implicitly in the good that is implanted in the human heart, I am convinced that none of the dire consequences foretold as the result of sex-determination will ever [xxi]happen. There will be no social chaos, such as has been darkly hinted, following on a birth-rate of nothing but boys, no mothers refusing to have girls or remaining sterile if they cannot bear boys. My own evidence goes to show that out of every hundred women who long for children quite 30 per cent. want nothing but girls, and 20 per cent. more are indifferent as to the sex of the longed-for child. All they want is to achieve motherhood under the most desirable and propitious conditions for infant and parents alike.
It is with all sincerity that I say that, from the very beginning of my studies, the sole object of my work has been to help women to avoid those special sorrows and humiliations which so often fall to their lot and to secure for them the privilege of choosing the sex of their offspring.
This book would be incomplete were I not to express my grateful thanks for the kindly advice and sympathetic encouragement which I have continuously received for the past [xxii]twenty years from many members of the medical profession. I would especially mention Sir Maurice Abbot-Anderson, M.B., B.S., M.V.O., etc.; Major James Taylor (of Keith), M.D., T.D., D.L., etc.; Edwin A. Neatby, Esq., M.D., L.R.C.P., M.R.C.S.; W. Ward Anderson, Esq., M.B., Ch.B. (Edin.); F. W. Lee, Esq., M.R.C.S., L.R.C.P.; and the late Dr. John Harley, formerly of Harley Street, London.
Cicely Erskine.
7 Eccleston Square,
London, S.W. 1.
[xxiii]
It requires considerable courage on the part of my wife, and not a little on my own, to face the publicity which a subject-matter of so delicate a nature as is contained in this work necessarily involves. Although the main essentials of the theory dealt with here were formulated over twenty years ago, it is only now that the progressive spirit of the age, in contrast with the prudishness of the last generation, has rendered it possible and desirable that mankind should have the full advantage of the knowledge of natural processes here disclosed.
Another more private and personal reason for withholding publication so long was the fact that our five children were young at the [xxiv]time, and it was obviously undesirable to ventilate this subject while their educational careers were in progress.
These impediments exist no longer, and the enormous power for good that must accrue to every potential mother possessing this knowledge far outweighs any possible disadvantages resulting from publicity. The author looks for her reward in the immeasurable benefit that others will derive from her unflagging inquiry and research.
The generous and self-sacrificing assistance that my wife has invariably afforded me throughout my public career renders insignificant by comparison, but none the less a mere act of gratitude, any contribution I have been able to make by way of encouragement in this, her life’s work.
J. M. E.
January, 1925.
[xxv]
| PAGE | ||
| Preface | v | |
| Introduction | xxiii | |
| I.— | Sex Determination | 3 |
| II.— | The Eugenic Point of View | 11 |
| III.— | The Selection of the Fit | 20 |
| IV.— | The Mothers’ Responsibility | 25 |
| V.— | Prematures | 37 |
| VI.— | The Superfluous Female | 51 |
| VII.— | Sterility | 65 |
| VIII.— | Sex-Causation | 77 |
| IX.— | For a Boy | 86 |
| X.— | The “Blank Week” | 97 |
| XI.— | For a Girl | 106 |
| XII.— | The Freak Ovary | 111[xxvi] |
| XIII.— | Lateral Decubitus | 120 |
| XIV.— | Signs and Symptoms: After-Effects | 131 |
| XV.— | Side-Theory | 141 |
| XVI.— | Twins of Mixed Sexes | 152 |
| XVII.— | “Before or After” | 163 |
| XVIII.— | The Length of Gestation | 173 |
| Appendix | 183 |
[1]
[2]
[3]
“Sex is the central problem of life.”—Havelock Ellis.
In reviewing the long and unenlightened past, one is tempted to ask whether Woman was not in league with the god of mystery to hide one of Nature’s simple laws from the knowledge and comprehension of man. Between woman and the possibility of instructive observation and the outward visible signs of its expression, there has seemed to exist an impenetrable barrier, so formidable as to baulk successfully every effort of the biologist. No doubt the educational system of bygone times contributed to the difficulties under which [4]scientists laboured in dealing with the problems of sex. It was practically impossible for maid or matron to allow her thoughts or conversation to stray from the beaten track without subjecting herself to severe reproof from Mrs. Grundy. A source of information was thus suppressed, for women as well as men have as much right to use their own understanding in judging of truth as they have to use their own eyes to see their way.
Now girls are allowed to learn, and encouraged to think, and women allowed to speak and encouraged to act. Thus we are at last approaching an explanation of the determination of sex, because, depending on woman, and on woman alone, it can be solved only with her assistance. “Life,” says Professor Lester Ward, “begins as female. Life is feminine. In the woman is the ‘creative centre.’ That everything proceeds from the egg, the ‘vital focus,’ is the verdict of Biology.”[1] In the ovum an egg alone is the germinal spot, the [5]dawn of the future life. The theory that the sex of a child is fixed before the ovum is fertilised has now become an absolute certainty as a result of thousands of successful tests which have established it. The male, according to science, is not a sex-determining begetter: he is simply and only a fertilising agent.
It is not necessary here to give a complete list of all the theories for sex determination that have from time to time been advanced. One by one, without ceremony, we can conscientiously demolish them, thus clearing the ground of useless impedimenta and narrowing down the difficulties to be overcome. Many of these theories were based on experiments and observations made on rats, bees, tadpoles, ferns, and even sponges. Then again the health, age, environment, habits, and diet of parents were successively advanced, apparently on the principle that any peg is good enough to hang a hat on.
Perhaps Schenk’s[2] theory beats the record [6]for extravagance, though it gained at one time many adherents. According to his curious doctrine, sex is determined during the months of pregnancy or well after conception has taken place. Surely as wild a proposition as endeavouring to grow a rose from a poppy seed by cultivating the soil in which it is planted.
This does not mean that there is no such thing as paternal heredity, in other words, that physical or moral characteristics do not descend from father to son throughout the generations. On the contrary, modern biology has demonstrated that a father does transmit any weakness he may possess to his progeny in a heavy percentage of cases, and more especially that the female members of a family will partake of this weakness; just as the mother passes on any tendency to disease or weakness of her own to her male offspring. These facts have a very important bearing on the transmission of disease, and it is obvious that the power of pre-determining sex would tend to [7]result in a strong and healthy race. If physical and mental deficiency in the male parent tends to be reproduced in the female offspring, and conversely in the male by a like deficiency in the female parent, it becomes simply imperative to ensure that in the former case only male children should be born and in the latter only female. A tubercular father need have little anxiety if he confines himself to sons only. A mentally deficient mother might without apprehension have a family of girls. With such possibilities open to us, we might even be willing to admit with Marcus Aurelius that “an accident is a misfortune, but bearing it well turns it to advantage.”
Since people who suffer from chronic disabilities will insist on producing offspring, let them at least make use of the essentially eugenic law which is offered here. Let them understand that henceforth, if they produce a specimen of humanity inheriting their own defects, they are alone to blame.
From time immemorial parents have accepted [8]in silence, but in bitterness of spirit, the advent of offspring of an unwanted sex. In 70 per cent. of these cases, it is roughly estimated, a girl has arrived when a boy was hoped for. In 30 per cent. only was a girl wished for and a boy born. Prayer without some kind of forethought must surely be unavailing. Help thyself, and Heaven will help thee. It would be of interest to turn for a moment to the East—to India in particular—and survey the conditions of life that prevail there. The abject plight of a great proportion of the women is largely the result of their lack of childhood, for among orthodox Hindus every girl must be married before her eleventh year; great numbers are married earlier still, some as soon as—if not before—they are born! The conditions under which the widows live—and these number over 20,000,000—are too tragic to contemplate, so trivial is their market value. In no country in the world is the Man-Child so ardently desired, for he is regarded as the Salvation of the household, as it is he [9]who will ultimately be called upon to officiate at the death-ceremonies of his parents, requisite for their re-birth, which to them represents their whole eternity.
In this great Dependency the mere whisper of sex-control evokes unlimited joy and enthusiasm among all who have heard of it and even faintly realised its possibilities.
Hitherto the ignorance of parents has been shared by a whole world of unobservant people, convinced “that the science of life and being is unattained and unattainable by these weak organs.”
That this helpless and hopeless outlook has resulted in the voluntary limitation of many families is illustrated to absolute demonstration by almost innumerable correspondents. “Were I to be sure of providing my husband with a son to carry on his name, I should most certainly bear another child” is a typical assurance. Most poignant in its pathos is the lament: “My husband refuses to let me start a child for fear it may be a girl, and my heart [10]is literally breaking for want of children.” Yet another epistle, several pages long, expresses the sorrows of an older woman, starved by an incomplete motherhood: “If only,” she writes, “I could make sure of a girl to be a sister to my three growing boys, I should willingly try my luck once more. But my husband absolutely refuses to have a fourth son to rear and start in life.”
Do not these extracts, which can be multiplied indefinitely, prove how essential is the choice of sex, in view of the perilous inroad birth-control is making amongst the classes from which we draw our best human material?
It behoves us, as human beings, to accept life with some degree of responsibility, not as animals pushed along the path of procreation by blind instinct alone. If, in the space of a generation or two, we have secured to mankind a better equilibrium of birth-rate, we shall have helped to make the world a far better place, and totally abolished that crying social evil “the superfluous female.”
[11]
“The destiny of organised nature is amelioration, and who can tell its limits?”—Emerson.
Eugenics is the Science of producing offspring of as perfect a type as possible, which must eventually result in the general betterment of the human race. So closely allied is moral welfare to physical that when the one is directly improved, the other, too, is proportionately benefited. “Ideals are the very soul of life,” and when they are high, the trend is towards progress. Unfortunately, between the theoretical and the practical side of all things there is a huge gap. The essence of practical eugenics lies in the application of rules, already in use for the benefit of domestic animals, [12]which, when applied to man, will bring about a higher physical standard than has hitherto been reached.
According to Professor Punnett “permanent progress is a matter of gametes, not of training—the man is not made, but born.”[3] Nature must therefore be helped in the creation of a finer and stronger human specimen by the selection of the fittest to fulfil the work of procreation. The diseased, the weak-minded, the consumptive and the crippled of the Universe would be prevented from producing offspring, and the race thus purged of necessarily inferior strains. The flotsam and jetsam of weakly humanity would die off after two or three generations, and but for sin and vice, which, like the poor, are ever with us, an utopian state of things would soon obtain. In other words, it only needs that human nature should be instructed and directed for all to be well with us, and eugenics, working on the principle that progress is a question of breeding [13]rather than of pedagogics, would accomplish what has up to now defied us as impossible.
Unfortunately eugenists are all too apt to forget how great is the abyss separating the moral from the animal being in man. Much can be done to improve the physique of a whole nation, but it must be remembered that “the character of a generation is moulded by personality.” Until the end of time the morale of a people will be the cause rather than the effect, and here alone lies the divine spark that animates our whole physical being.
A happy antithesis to Eugenics is to be found—the science of psychotherapy, the essence of which has been summed up in the words, “It is fatal to trust in the squirrel-work of the industrious brain, instead of the piercing vision of the desirous heart.” Here the moral being of Man is placed far above his physical or even mental being, which are in more or less complete subordination to his soul, according to the degree of his spiritual development. [14]Heredity is disregarded as a negligible quantity. It is environment, suggestion, willpower, faith, that wholly influence, compass, and direct the well-being of man.
With eugenics, on the other hand, heredity is the most potent factor, and this is perhaps why the key-note of materialism runs through the whole gamut of this idealistic striving towards a more flawless humanity.
Heredity allows for little freedom; so it must be curtailed. Human nature must either be completely held in check, or transformed beyond recognition. A check is provided by the simple method of isolating those human beings who, as a result of disease, are unfit to bear or beget children. Thus in time the birth of mentally deficient creatures, who are prolific out of all proportion, would come to an end, and other forms of inferiority might in time be enormously reduced, and finally eradicated.
So far, so good, but there are other whisperings in eugenist circles, and particularly in [15]their outer fringes, which deal with subjects so intimately human and personal that one is inclined to question the wisdom of attempting to rush in where angels have feared to tread. It is, for instance, not unusual to speak of the perfect mating of two physically superior beings who should produce perfect offspring. But so conspicuously inconsistent is human nature that often a healthy man will fall hopelessly in love with an inferior or even physically degenerate woman, and vice versa.
Then polygamy is hinted at; the strong man, as in Eastern countries, may remain mated to his love, but should wed another wife who will produce fine human stock. So, after a war, the strong man who survives will have two or even three wives to ensure the future welfare of the world. Such proposals have latterly been mooted by more than one writer, with so-called eugenists foremost among them. The decisive answer to all such schemes has been given in advance by Montesquieu, in his great work L’esprit des Lois. Very minutely and [16]conclusively he has proved that polygamy never did, and never will, accomplish the desired end, and that it is invariably accompanied by race degeneracy and both mental and moral deterioration. It has appealed to some of the oldest civilisations all the world over, and, after devastating wars, plagues and famines, has been solemnly tried and encouraged. But from the national point of view, polygamy does not answer.
Family life, with all that it implies, is primarily responsible for the healthy moral and physical upbringing of normal human beings, and true family life can only exist in a state of unimpeachable monogamy. One father and one mother, welded together in a common desire to work for the good of their children, can alone produce a truly healthy and superior race.
In polygamy wifehood becomes a farce, and motherhood a mere animal function, generally limited to a single attempt, and followed usually by a state of lymphatic inertia and [17]gross self-indulgence. The parental instinct here is blunted on both sides, and all that can reasonably be looked for in an institution so closely resembling the farmyard is a purely physical relationship between man and woman, mother and child. Marvellous results have been achieved in animal breeding by the coupling of superior males and females singled out for the sole purpose of providing superior progeny. As regards humanity this can never become a feasible condition and polygamy remains a form of barbarism or gross degeneracy. Turkey gives us a fair example of civilised polygamy. In her essay on the harem, Lady Cook describes the Turkish woman as being “the most depraved in the world.”[4] My personal experience of Turkish society, which is not slight, has led me to a similar opinion; indeed, the results of polygamy on the race where it is practised to-day are too obvious to require further comment.
Shortly before he died, Mr. Montague [18]Crackanthorpe, the eminent Eugenist, in a discussion on this subject, remarked, “There is no doubt that animal life, in its natural state, is essentially monogamous. How much more is man then by nature, let alone by civilisation, intended to generate after the highest form of monogamy.”
It has been proved too often to admit of doubt that the moral influence of the mother on her unborn infant is omnipotent. Prenatal sensations may well account for the whole trend of the child’s life. In the words of Dr. E. Sloan Chesser: “Socially, the mother is the basis of racial progress: ethically, enlightened motherhood is the strongest force in the world. Intelligent mother-love can alone bring about the inculcation of higher ideals of citizenship and social obligations.” The need of the hour is the training of mothers in the deeper questions of life, so that the new generation of men and women may have a sane and strong sense of human responsibility and a better understanding of international morality [19]and friendship and the unity of the human race.
Much can and should be done by encouraging those who are fit and healthy to have larger families. The Malthusian theory has proved itself a dangerous menace to civilisation. It is threatening the safety of depopulated France, and in Great Britain it should be discouraged in every possible way as an insidious and treacherous enemy to the laws of God and man.
[20]
In every kind of animal life, with but few exceptions, the males exceed the females in number, so that for the female the field of choice remains a wide one. Among birds it is the cock who acquires the outward adornments of feathers and the sweet singing voice wherewith to woo the hen. She, in her turn, selects the mate she prefers to help her build the nest which is to receive the offspring of their union. Similarly, various kinds of animals, when the mating season approaches, acquire new fur or horns to help them with their courtship.
[21]
With us it is otherwise. In the civilised countries of to-day it is the female element which exceeds the male, so that the choice of a mate lies necessarily with the latter part of the community. The woman is compelled to show some special advantage, whether beauty, wealth or some other feature, which will make her peculiarly desirable to the man she wishes to attract. For this reason we often see women lose their self-respect or indulge in the most absurd extravagances in the hope of distinguishing themselves from the mass of their own sex. In the poorer classes, this condition prevails only to a minor degree, and for purely economic reasons nature has her own way to a greater extent. But even here, as everywhere, women are far too prone to take what they can get, rather than remain unmarried. We still find the loafer, the diseased and the drunkard, if like Barkis, they be willing, turned into benedicts, almost before they realise it themselves. Hence the heavy percentage of imbeciles, cripples and degenerates which burden the country [22]and fill the lunatic asylums, hospitals and prisons. This unfortunate condition is due to the fact that in the British Isles there are, according to the statistics of the Registrar-General for 1923, at least 107 women to every 100 men.
More men must be provided to ensure offspring as perfect as the human race can create. Once the heart and imagination of the woman are satisfied, she will spontaneously fulfil her great rôle of mother. Thus equipped, she will carry on her work conscientiously, fully alive to the importance of her child’s welfare. It is the mother’s morale that counts in reproduction: she takes the giant share of the responsibility.
She represents the Sex, self-contained and all-containing; Le sexe, c’est la femme. And yet, in preparing for the ordeal of motherhood—the pivot on which the whole world revolves—her chance of selecting a partner, worthy to become the father of her children, is comparatively small.
[23]
The wonder is that more unhealthy children are not born as the result of such a limitation of choice. By the subsequent exercise of great care, many are reared to become useful citizens, but a vast army of permanent inefficients is born into our midst every year. In a population of 40,000,000 there are 300,000 mentally defective persons, most of whom are in asylums, but many still free to marry and procreate. Thus one person in every 118 of England’s population is either mad, idiotic or feeble-minded. Among criminals alone, the fruit of degeneracy, there are in England 30,000 in the jails, besides some 5,000 classed as convicts. There are also every year in England and Wales some 3,800 people who died by their own hands. All these degenerates contribute but little benefit to the State, which is in fact often called upon to support them and their offspring entirely.
In these years of progressive enlightenment it should, above all, be recognised that the general welfare of the nation is immediately [24]dependent on the common sense and morale of its women. It is of primary importance that they should make use of all their intelligence and all their forethought before embarking on the hazardous venture of matrimony.
[25]
“The only science of mankind is man.”—Warburton.
We have spoken of the advantages to be obtained from a eugenic point of view for women and their children by providing a larger selection of suitable males. But we must not forget how innumerable are the influences which can affect the unborn infant. It has been asserted that the phlegmatic and lazy woman is more prone to female offspring, whereas her sanguine, hardworking sister is usually blessed with male children.
There is a reason for this. The natural state of every healthy woman is to produce more males than females. In Russia, where the peasant-women do heavy manual work on their [26]homesteads, the percentage of male births far exceeds that of female. Among the French peasantry the same condition prevails. During the war it was commonly acknowledged that the male birth-rate increased greatly. When one bears in mind the enormous amount of hard physical work that was accomplished by women, who otherwise would have led a sedentary, or at least a far more passive existence, one can hardly be surprised at it. For this unusual outlay of muscular energy resulted in the strengthening of the whole right side of these women, and incidentally of that organ from which male issue springs.
Most decidedly it takes a stronger and more normal organism to bear male progeny than female. Regular work and exercise, combined with favourable moral and physical conditions, are necessary to the conceiving of boys. There should be no exaggerated zeal in the pursuit of sports and games, but a wife should take a moderate part in all her husband’s pleasures and occupations, and reserve enough leisure [27]to ensure a tranquil and contented brain. To keep cheerful and happy is half the battle for the unborn infant.
A lady I knew, who had thirteen sons and two daughters, was so strong and muscular that up to the age of 85 she could take a very active part in any furniture-moving that had to be done. A friend of my mother’s, who had twelve sons, remarked one day, “I think I ought to have been a man, I am so much more muscular and powerful than my husband.”
A certain amount of intellectual activity is desirable, such as reading, music, or any form of accomplishment hitherto cultivated. Any talent to which active expression is given during pregnancy greatly affects the unborn child, in whom the seeds of so-called facility, talent, or genius are thus sown. Once pregnant a woman should never forget for one minute that her burden must be considered at every step she takes, just as later on she will hope to watch over her infant’s welfare at every hour of its existence.
[28]
Much can be done to ensure the safety of pregnancy, especially during the first four months, by early hours, easy-going occupations, and above all no giving way to worry, morbidity or temper. A morbid mother produces a fretful baby, who may quite possibly develop a “kink” in his brain or character. Here also should be underlined the necessity of guarding against the fatal catastrophe of miscarriage, only too often brought about by sheer carelessness.
The following are a few typical cases. A lady of my acquaintance, when pregnant, was in the habit of riding in the Row every morning, up to the sixth month. Three times in succession the child was a girl, and no apparent trouble ensued. When, however, she became pregnant a fourth time, I warned her against the risk that to my mind she was incurring. But she continued to take the same exercise, and shortly after she miscarried of a boy, which proved to be her only attempt at male issue.
A young woman who had a boy of two years, [29]and was pregnant of a second child, insisted, in spite of all the friendly advice offered to her, in going to Switzerland for the winter sports. She skied all day and danced all night. Shortly after she became ill, was seized with pains, and miscarried of a four-month boy.
A lady, who already had a daughter, much needed a son to carry on her husband’s title. She became pregnant, and went comfortably on till the fourth month, when, at the time when quickening was due, she was invited to join a party to go on a long excursion in a coach-and-four. Though warned beforehand by all her friends, she persisted in accepting the invitation. She came home worn out, and miscarried next day of a healthy male fœtus.
A lady, who was inclined to feel ill for two or three days each month, was warned by her doctor to lie up at these times. She insisted however, on one such occasion, in taking a long train journey, with the result that pains came on, and she was delivered of a four-month male child.
[30]
Another correspondent recently wrote:—“I started a baby immediately after marriage, but stupidly did far too much and had a miscarriage in July and another in December last.”
On the other hand, many of these mishaps may be due to unavoidable accidents, shocks, and mental worry. But this only emphasises the desirability of avoiding all imprudence at the first suspicion of pregnancy, and of using the greatest foresight and self-control when there is any smallest symptom of “bearing-down” or “malaise.” The old saying, “A sick pregnancy is a safe one” is doubtless true.[5] But sickness would appear to be more prevalent in girl-pregnancies, and this goes far to support the fact of partial immunity in pregnancy from female abortions.
A lady pregnant of a boy wrote to me as [31]follows: “I am not a bit sick this time ... but with my first and second babies (both girls) I was terribly sick and could keep nothing down for weeks on end.” A lady in Paris assured me that with her four girls she suffered very greatly from nausea, but that with her two boys she was free from all such discomfort. A woman who had eight daughters and four sons told me that she invariably knew of which sex her baby would be, as sickness was always present during the first three months of girl-pregnancies. Of such cases I could quote many instances.
Here let me say that miscarriage is one of the direct causes of a lack of males in the world. Statistics show that of the miscarriages within my own experience no less than 80 per cent. are male. To this I must refer later on.
There are other causes responsible for the dearth of boy-babies, all more or less capable of adjustment. For instance, the fact that it is more difficult to rear boys depends on two [32]special causes. The first is the boy’s digestion, which, in my opinion, is more delicate than that of a girl. This I have noted in hundreds of cases, extending over many years, and certainly boys are more inclined to sickness than girls. An elderly monthly nurse of great experience used to say, “my sick babies are the fattest and the biggest, and are generally boys,” and she always maintained that “small babies” were easier to rear than big ones. A mother of ten children recently remarked to me, “My girls were no trouble, but the boys were so difficult to suit with their foods.” This is a matter of experience which I have confirmed in countless cases.
Therefore it is all-important that boys should be breast-fed, if only for the first month of their existence. For the after-health of the mother, wishful of further male issue, this is also very desirable. The infant’s best chance of life and health is that it should be born of a robust mother capable of nursing her child during the first months of its existence. [33]Walsh, in his work on Psychotherapy says, “It is well recognised that the reason why nurslings are protected from most of the so-called children’s diseases is that their mothers have had these diseases, have acquired an immunity to them, and this immunity is transferred to the child so long as the nursing process is continued.”[6]
Every mother should, therefore, endeavour to take plenty of nourishment, so that she may be able to feed her child as long as possible. In order to be successful, a quart of rich milk should be taken daily; there will be no difficulty in digesting this, so long as she continues to nurse. Beer and stout, however, have been proved to be unnecessary and often harmful for the creation of pure milk. To show how important it is to nurse babies, it is only necessary to state that in London alone during the summer 200 infants die every week from “hot weather” diseases, in most cases propagated by flies which poison the milk.
[34]
The second cause of boy-mortality is the widespread, and often ignored, necessity for circumcision. Every male infant should be circumcised within the first week of its birth. If properly attended to, the child does not feel the slight operation, and naturally no anæsthetic is used. Circumcision is an insurance against many troubles later on. It is cleanly and a real safe-guard to morality from early boyhood upward. Every child thus attended benefits thereby, and it is especially desirable for children of neurotic or tuberculous parentage. It has been remarked that the Jews rear a much larger percentage of boys than do Christians, and there can be no doubt that the circumcision universally practised among them is one of the chief causes of this smaller mortality.
Anæsthetics must be resorted to if this operation is performed later on, and this, in itself, always entails a slight risk. Otherwise I hardly know a single case where any serious degree of trouble has arisen from circumcising an infant. [35]On the contrary, I have seen great relief afforded by the operation. The number of cases is increasing yearly, and facilities should be extended to all classes for obtaining this necessary surgical treatment for their babies. Public opinion should be educated as to the great necessity of this operation, and, just as vaccination is compulsory, so should circumcision be looked on as necessary to the physical welfare of the male child.
With the advent of women into public life it was realised that their special profession of motherhood had not been adequately assisted or safe-guarded. Even before the war broke out, Government help was offered in the form of a grant to defray the expenses of local health work. As a result, England is now saving 50,000 babies a year, who would formerly have died. In other words, we are losing one in eight instead of one in seven, and the death-rate is proportionately lower.
During the great war England lost, every hour on the battle-fields abroad, ten men. At [36]home every hour twelve babies under one year of age die. We could not save the men abroad, but we may well save as many of the infants at home. And it is the patriotic duty of every woman to help preserve the babies—the nation’s greatest asset.
[37]
“There is no true potency, but that of help; nor true ambition, but ambition to save.”—Ruskin.
There existed long ago in Paris, in the Boulevard des Capucines, an institution called “La Couveuse,” where, on payment of a franc, one could see an exhibition of babies, domiciled in incubators for the period of time requisite for their complete development. I do not know if the same place is still in existence, but when I saw it, it was a long room divided by a corridor with half a dozen incubators on either side.
Each of these was tenanted by a wee premature baby, which had made its appearance [38]at least two or three months before it was expected. More than half of these infants (they were mostly boys) had enjoyed an embryo existence of just six months. They had, as Shakespeare puts it,
These babies were fed by three or four “nourrices,” who lived on the premises and supplied each little incubated person with a drop or two of human milk administered in a teaspoon, as none could suckle until the end of the seventh month.
Among these infants a little pair of red-haired twins, born at twenty-six weeks, were especially attractive. Their name was Smith, and they certainly had a familiar John Bull-like expression of countenance. Their native vigour proved itself in their obstinate battle for life. Two years later I was able to see those same twins in the best of health and spirits, and to all appearance as bonny specimens [39]of humanity as any parent might desire.
Hitherto incubators had been regarded solely as a means for hatching chickens. It was in France that Dr. Tarnier for the first time applied the system to the rearing of weakly babies. At the Maternity Hospital in Paris, and in various other places in France, “couveuses” have now been employed, for over twenty-five years, with the greatest success. It seems a pity that in Great Britain the incubator is not more widely used. Perhaps on account of the antipathy shown in that country to the wet-nurse system, artificial feeding is a stumbling block. It certainly is almost impossible to rear an infant born at six months on anything but human milk. Wonderful results have been obtained, thanks to the incubator and human milk combined, while many thousands of invaluable boy-lives have been sacrificed for the lack of combined artificial warmth and proper feeding.
Personally I know of no less than eleven little six-month prematures who could have [40]lived and thrived, had an incubator been available. One case in particular was heart-rending, as the tiny creature cried pitifully for nearly twenty-four hours on end, as if begging to be saved. Born at six months from the last day of period, he was well made, with a voice as strong as any full-time infant’s. Unfortunately it was bitter January weather, and no amount of hot water bottles could keep the cold air from his little lungs. He died the following day, literally perishing with the cold, and worn out with his struggle for life. Here was a case where an incubator would have solved the problem of rearing successfully a perfectly healthy atom of humanity, thrown into the world before its time, owing to the fact of its mother being elderly and not of a very robust nature.
A medical friend of mine told me recently that, had he been able to procure an incubator, he was sure his own seven-month baby girl could have been reared. Twenty-five years ago an attempt was made to introduce [41]them in England, and I know personally of two mothers who made use of them with success. In one case a very tiny seven-month girl was put in an incubator for two months, and has grown up to be a fine healthy young woman. The other did equally well, and is, I believe, still a woman of strong constitution.
Why the use of incubators did not become more general was evidently because they were difficult to procure and expensive to hire. Then the question of food without the wet-nurse system renders them very difficult to use privately. But there seems to be no reason why these difficulties should not be overcome in hospitals and private “Homes” where so many premature, or difficult, lying-in cases are to be found. Wet-nurses doubtless could be obtained, and, if this were not possible or desirable, humanised milk or some patent food administered, with effective, if not equally excellent results.
As a rule I do not hold with the wet-nurse system; it has been tried for generations and [42]found wanting. The moral question is at the bottom of the failure. Perhaps also the eugenic point of view had something to say about the transmission of hereditary taints through the milk of a foster-mother, quite frequently drawn from the lowest stratum of society. In the last generation, of course, the use of wet-nurses was an habitual occurrence with the well-to-do. But then it was a common question whether the child did not often become similar in ways and even looks to its foster-mother.
My own mother, who had ten children, of whom four had wet-nurses, used to remark in her latter days how much these children partook of the robust health and nature, and even looks, of those who had nurtured them. In the case of one of my brothers this was especially marked, and it was also certainly noticeable in one of the girls.
In France, where many children are put out to nurse, the disadvantages outweigh the beneficial results of human lactation. The nurses [43]hold such a sway over the mothers, and in many cases abuse the power they control to such an extent, that the mother’s care is discounted; her maternal instincts are blunted, and the child, once weaned, becomes the defenceless victim of ignorant incompetence and wrong feeding. Meanwhile, the nourrice returns to her native village to find the child she left as often as not a puny weakling, suffering all the evils of maternal neglect.
Nevertheless, if a wet-nurse were immediately available, she would accompany the promptly forthcoming incubator when required, and many thousands of premature male lives could be saved. I say male advisedly, for the reason that a six-month baby is nearly always a boy, whereas the rare five-month miscarriage is generally a girl. In April, 1915, at Sunderland, England, a Mrs. Pallion, the wife of a soldier, gave birth to premature boy-triplets. They were immediately conveyed to the Children’s Hospital and placed in incubators. They have all survived and [44]done well, and were duly christened Kitchener, Jellicoe and French. The public can hardly realise the enormous number of children lost to the nation as a result of still or premature birth.
As a rule no fœtus is born viable before twenty-six weeks, though according to Scotch law, an infant may be viable at six lunar months or 168 days. A Mr. Tait reports a case in which the mother gave birth to a girl at five months and twenty-seven days. It lived four months. Dr. Keiller recorded particulars of a case in which a child of about four months intra-uterine life lived for about an hour. It weighed 9½ ozs.[7]
Under ordinary conditions it is almost hopeless to try and save these mites; but, if the greatest care is exercised, it is nevertheless possible to rear a goodly proportion, in spite of the many difficulties. Here is a case in point from my own experience: A Scotch woman, over forty and very stout, gave birth [45]to a seven-month girl, her first-born. She reared it with trouble owing to her inability to nurse it. Nine months later she became pregnant of a boy, which was born barely over the six months. A day after its birth, when weighed, it turned the scale at 1 lb. 10 ozs. The doctor present did not think it would survive. It seemed impossible to keep the infant warm, as it had no powers of suction.
When asked to take over the baby, my first care was to wrap him in cotton-wool and flannel, discarding the cotton shirt in which Highlanders invariably swathe their shivering offspring. I next secured a rubber hot water bottle, filled it with warm water, and baby and bottle were rolled up together in a blanket. The next problem was how to feed it. The mother, happily, had plenty of milk this time, and by means of a teaspoon I drew off a few drops at a time and fed the baby every half-hour. He stopped crying and slept for hours on end. The bathing difficulties were great, as he was so tiny as to fit into my hand, and [46]his little legs were about as long and fat as my finger.
After seven days of this system, in which I was helped by the devoted and painstaking mother, the infant had gained 6 ozs. and began to look almost like a real baby. At the end of three weeks, during which time we just managed to keep the mother’s milk-supply going, the child was able to suckle all he required for the nourishment of his minute frame. By that time he weighed 3 lbs., and had acquired a good hold on life. For three months he lived and slept with the hot-bottle, and at the end of that time he weighed 7 lbs. At one year he weighed 20 lbs.—well above the average weight—and, as I write these words I recall that he has grown so big as to need “breeching,” much to the satisfaction of his excellent Highland mother.
The moral of this story is that if a hot-bottle and mother’s-milk could save such a “puir wee loon” as that recorded above, thousands of babies in similar plights could be saved yearly. [47]The whole care consists in the proper warming and feeding of these premature infants who need to be literally coaxed into remaining with us in this cold and hungry world. In New Zealand, state and voluntary efforts have united to provide what is, judging by the results, the most perfect system for the care of maternity and infant welfare that the world has ever seen. A voluntary society has management and control of the whole work. No money grant is made, but aid is given in skilled attendance, advice, and teaching. In five years the infant death-rate has fallen from 80 to 35 per 1,000, whereas in Australia it still stands at 71. It is significant that this marvellous superiority in the numbers of children reared in New Zealand dates from the time that women were given the vote.
In England in 1914 the death-rate was as high as 108 per 1,000 births. In 1924 it was only 69 per 1,000. In twenty-five years it had been reduced from no less than 150 per 1,000 to 69. There are now 2,200 infant welfare [48]centres in the country, and 2,650 women employed on infant-welfare work.[8] In Germany, France and Italy, the death-rate of infants is terribly high, and in modern Greece only one child in three survives to its first birthday. The reasons alleged for this state of affairs are the sudden changes in the fickle winter weather, and the amount of soft fruit with which babies are generally fed in summer-time.
As regards the death-rate from causes connected with maternity, there has been a great improvement in England since the passing of the Midwives Act. There are now 135 maternity hospitals and homes, and, whereas 20 years ago, five mothers died for every 1,000 children born, the rate has now been reduced to less than four. With the advent of the new method known as “Twilight Sleep” or painless childbirth, and the numerous other means of ameliorating the condition during confinement, no woman need dread the ordeal of childbirth, [49]but can look forward with unmixed joy to the advent of the child of her desire.
The excess of boy-births over girls has been recorded in Germany, France, and England for more than 200 years as being at the rate of 106 boys to 100 girls; but against this we have to reckon with the greater mortality of males already described, which, of course, does not include the death-rate causes connected with men’s several callings, e.g., the army, the navy, mines, colonial pioneering, etc. I have enumerated the many ways in which we can help enormously to reduce male infant mortality, and that surely is the first and most important step. In 1916, it was calculated that in Australia, 72 babies died out of every 1,000 born before reaching twelve months of age; in Norway 72, in Sweden the same and in Holland 99, in the United Kingdom 109, in France 120, in Germany 170 and Austria 205. But in New Zealand, where women take an active part in public life, only 35 babies die out of every 1,000 born. These figures tell [50]their own story. Where women have most power, the infants have the best chance of living.
Where women do not count in politics, the babies have the worst chance. And where all babies have little chance, the boy-babies have by far the least.
It is true that we have made great strides in the direction of infant-welfare. But very inadequate progress has been achieved with regard to the saving of the thousands of premature boys, who die every year, when they could, given the help of incubators and special feeders, be fostered and reared with entire success. I have explained that six-month prematures are almost invariably boys, just as the five-month child is nearly always a girl, and though it may be impossible to save the latter, I have endeavoured to prove that it is well within our powers to accomplish apparent miracles in preserving those male atoms of humanity. They need not die, but may grow up to become healthy and useful citizens.
[51]
“Life begins with the female organism and is carried on a long distance by means of females alone.”—Lester Ward.
The old saying that girls are easier to rear than boys has been already referred to and commented on, and its truth has been established by statistics. It is true also that girls are easier to carry through the period of pregnancy.
One reason is that they are carried higher in the uterus than boys, so that serious bearing-down feelings are rarely experienced in girl-gestation. Doubtless, too, the greater pressure upwards against the digestive organs accounts for the more frequent nausea experienced during girl-pregnancy.
[52]
In most cases where hitherto hopeless sterility has been relieved it has been through the birth of a daughter—“Nature’s weakest growths have quickest spring.” In the far fewer cases where a boy has been born, the former sterility has generally been due to some slight anatomical disability rather than to any local delicacy or disease.
A powerful proof of the safe pregnancy of girls lies in the fact that girl miscarriages are of very rare occurrence. Out of every hundred babies who miscarry, as I have already noted, eighty are boys. Among fifty letters received recently from women who wanted sons, no less than eighteen spoke of mishaps of four-month male children, two mentioned miscarriages with a female at five months, and in eight others miscarriages during the first few weeks had occurred or were suspected. Doubtless a vast number of male abortions occur at or about the third month and at a time corresponding to the menstrual period.
[53]
Female abortions, on the other hand, generally occur at the end of the fifth month, possibly as the result of shock or accident, but more commonly owing to disease. They are often caused by a syphilitic condition of the womb, or by a tainted father. In Aberdeen I noted a woman who had given birth to two healthy boys, but with her first-born—a girl—she had miscarried at five months; her husband suffered from syphilis. In another case a woman produced a healthy boy, but the next child—a girl—aborted at five months. I have collected numerous cases of girl-miscarriages happening at the same length of fœtal existence, and all due to severe accidents or abortive methods, when they were not the result of a syphilitic condition.
There are innumerable cases to prove that a hereditary taint on the father’s side is more likely to affect his daughters than his sons, provided the mother is healthy. In the case of a Viennese family, I noted that the two girls both showed the signs of a tainted father, [54]whereas the three boys were as strong and healthy as their mother.
A case in which I was much interested was spread over a number of years. It was that of a poor country woman, who, when I first met her, had a healthy family of four girls and a baby boy of ten months. After that she gave birth to a girl who wasted away at two months with some tubercular trouble; from that time on the mother had continuous pains in her left side. However, at the end of a year, she was confined of another tuberculous girl who lived only eighteen months, and ten months later still she gave birth to yet another girl-child premature and still-born. After this the poor mother became seriously ill. The pain in her left groin was almost unbearable, and continuous discharge caused her at last to seek surgical advice. At the end of some months of drastic treatment for tubercular trouble in the left ovary, the patient was completely cured, and two years later she gave birth to a little son. Though [55]apparently free from disease, he was rather small and weakly and, when a year old, died of whooping-cough. But a year later the mother, having now become a robust woman, produced a fine and lusty boy who is now nearly four years old.
The explanation would, I think, be as follows. The father, a consumptive-looking man with a tubercular family-history, transmitted the trouble to his fifth little girl, who in her turn infected her mother’s left ovary, and it was only after the birth of two more sickly infants that the disease became acute. As a result of the surgical removal of the diseased left ovary, the woman was left with a single normal right ovary, which was brought into renewed activity by the extinction of its rival; hence the birth of the two sons.
Here is another case which goes to prove that a son will readily inherit a disease latent in his mother. An apparently healthy mother bore a son who soon developed symptoms of the chronic asthma from which he still suffers. [56]Five years later the same woman bore a healthy girl, and finally two years after that she again became pregnant, and showed symptoms, for the first time in her life, of distressing attacks of asthma. After giving birth to a healthy girl, she died of exhaustion caused by one of these attacks. Here it will be observed that the boy alone partook of the latent maternal disease whilst the baby-girl, like her little sister, has grown up quite strong and healthy, and entirely free from the complaint.
Then again the extreme rarity of the premature dislodging of a female fœtus tends to prove that:
1. A more or less healthy womb will harbour a girl-child; whereas it requires a very strong and vital uterus to carry a male to its full term and viable. Thus a lady writer:
I have to lead a very quiet life and I am very anæmic; each of my babies—I have three little girls—arrived two or three weeks too soon. My period is very profuse, and always five days “early”.... I wish I were stronger and could bear a son.
[57]
Another letter runs thus:
I am terribly anæmic, my periods always “early” and far too profuse.... I have had four girls; none of their births were normal.... I had an operation to my bowels after the first; severe colitis after the second; and had to be curetted after the third; and since the fourth confinement I have been very ill and have had my appendix removed. My doctor told me I was not the type to have boys, as I am very small and delicate especially internally.
2. In very many cases, female children are born to any given selection of couples who otherwise would not have parenthood. It is unfortunate, but I can count on my fingers the cases of obstinate and apparently hopeless sterility that have been relieved by the birth of a boy. In far the majority a girl has been the result. Lady B. wrote as follows:
I have been married many years, and have never had a sign of the child for which I long.... The doctors tell me I am fearfully anæmic, and nothing I do seems to help....
She was a very nervous and excitable patient, and gave me much trouble for many [58]months. Finally she became pregnant immediately after the period, and in time produced a fine healthy girl. I have not kept trace of her history, but I do not think she has had further offspring.
3. Since so many women are inclined to produce one child only, and since miscarriages are more common among male children, there is a large predominance of girls as first or only children. I have collected statistics of hundreds of such cases.
4. There are more sets of girl-twins born than boy-twins; since the former, being easier to rear if premature, more easily survive their birth. Similarly in twins of mixed sex (and these are of more frequent occurrence than any) the boy is the more difficult to rear than the girl.
A usual form of in-breeding in human beings or animals is the predominance of female progeny. This is especially noticeable with toy-dogs of various descriptions; out of every litter there may be only one male dog, frequently [59]none. I have heard several complaints on account of this anomaly. In pedigree “catteries” the same condition has been freely observed.
In Turkey there is a vast predominance of girls born, and the death-rate amongst boys is stupendous. Though all the women are married, it is rare to find anything but small families among the well-to-do classes, and where there are many wives, one child apiece is the usual result.
It is now becoming more generally recognised by students of this branch of science that the first child is usually inferior to the second or third, and accordingly, when a nation is largely composed of enfants d’essai, as the French call them, race degeneracy and possibly even depopulation are not far off. This explains why the one child system has proved so calamitous to a country like France, which is vainly struggling in the vice-like grip of the Malthusian theory.
Another evil closely concerning the birth-rate [60]of females is that of illegitimacy; many more girls than boys are born out of wedlock. In 1922, 60,000 illegitimate infants were born in Great Britain, and among these there were 106 females for every 100 males, which is almost exactly the reverse proportion of the legitimate birth-rate. For this state of affairs there are several reasons:
1. Large numbers of them are first children, and of these 70 per cent. are girls.
2. In such confinements too little care is generally given both to mother and child, and the male child, having a larger head and being therefore more difficult to bring into the world, is frequently still-born. That, moreover, half the still-born children are not registered, may further help to account for the disparity.
3. A male abortion is fairly easily brought about, but female issue is infinitely more difficult to get rid of.
4. Illegitimate children have obviously less chance of surviving than those born in [61]wedlock, since their upbringing is necessarily rather irregular. Boys succumb more readily than girls to the evils which attend upon their undesired presence in an unfriendly world.
And here, by way of digression, I would point out that much misconception prevails regarding the normal prevalence of illegitimacy in England. It is not necessarily the product of either poverty or of city life. It is far more common in rural districts than in urban areas, and, even in cities, it is by no means the poorest parishes that produce the most illegitimate children. The urban artisan class as a whole is far more rigid in observing the sanctities and prescriptions of marriage than any other section of the community. In the country there are many more families who live comfortably with the illegitimate baby in their midst, and only a minimum of shame or compunction is experienced either by the mother or grandparents.
The fact that some 60,000 illegitimate children [62]annually appear in England is well calculated to destroy some of our pharisaical complacency. In such a godly country, one would somehow have expected better things. It is true that in Germany, where the population is to that of England as 5 to 3, the illegitimate births are as 5 to 1—and that in Austria, the illegitimate birth-rate in 1916 was as high as 50 per cent., but both these countries, like many others, are burdened with impossible marriage-laws, and many are the obstacles in the way of a legal union for every citizen, rich or poor.
“God sends not ill; if rightly understood, all partial ill is universal good.” We must economize our babies; whether born in wedlock or out of it, every child has a right to some share of our consideration, and every mother, whether married or single, should have the right to demand such care as will save the children she bears from death in infancy.
It is estimated that 70,000 children are actually still-born each year, and there is little [63]doubt that a very large proportion of these could be saved by a national scheme for the protection of mother and child. What we need is a kind of institution which would ensure that undesired male infants were privately removed from their surroundings and brought up under proper supervision and care. Thus only could we save the greater part of those boy lives at present thrown away, and which ought to go to fulfil the needs of our under-populated dominions, crying for settlers. The girl-babies could more safely be left with their mothers, or to the hazard which seems to regard bastard girls more kindly than boys.
It may seem something of a digression to add that, with regard to the causes of illegitimacy a very potent factor might be found in the countless public-houses of every town and village in the country. Remove excessive drink, and two-thirds of the immorality in the world will likewise disappear. This would prove especially true in Great Britain, where [64]the ideals of morality are high, and religion is still a real safe-guard.
Shakespeare said: “A man who goes to bed drunk begets a daughter.” Whatever the theory on which he based this assertion, there remains very little doubt that many unwanted lives are brought into existence as a direct result of over-indulgence. It has often been stated that the ill-kept public-house is one of the greatest disseminators of consumption. How much might also be said of drink in connection with the spread of venereal disease!
But my main point is that intemperance means a high illegitimate birth-rate, which in its turn is the direct cause of the preponderance of girl-babies which survive and so accentuate this unfortunate disproportion.
[65]
“Sterility does not necessarily prove that the sexual organs or functions in either the male or the female must be in an abnormal condition.”—A. W. Eddis.
The causes of sterility are so multiple and diverse, and such countless volumes have been written on the subject, that I do not consider it necessary here to enter fully into all the particulars connected with the condition. According to Chavasse one wife out of every eight is barren, and the majority of these are to be found among the richer members of society.[9] Mr. Arthur Eddis reckons that in Great Britain alone there are over 500,000 sterile married women.[10] Only 7 per cent. of [66]the fertile bear their first children after the third year of marriage. Therefore, if the first year has gone by with no sign of pregnancy, the young wife should bestir herself to examine the possible causes of failure in this direction.
Dr. Marion Sims, who devoted much attention to the treatment of sterility, laid down several general rules as essential to fecundity. One of the most important is that “Semen with living spermatozoa should be deposited in the vagina at the proper time,” or, in simple words, healthy fluid or seed from the male should be deposited at the proper time in the passage of the female. Now it may seem at first sight extraordinary, but many a childless couple remain so for the simple reason that never once in their connubial life have they hit on the suitable day on which, rather than any other, they could beget offspring. And that is precisely why so much help can be obtained from a suitable choice of days.
One lady I was asked to treat had been [67]married nine years and at thirty-eight still remained childless. She was a healthy woman, but had complained of severe pains in her back and right side at certain times. Her periods were regular, so that it was easy to ascertain and utilize the day before the period was actually due. A slight flow ensued, but stopped on the third day—the patient went off to the seaside immediately and stayed there alone for some time. In three weeks she experienced much nausea, and the usual signs of pregnancy were soon detected. At the end of nine months from the day mentioned, she gave birth to a very fine little girl.
I would like to emphasise the marvellous effects of sea-air on the health of certain women. I have known the most obstinate childlessness cured simply by four to six weeks spent by the seaside.
A lady came to see me once who had been married for fifteen years without—so far as she knew—having ever conceived; she was over forty, her health was indifferent and she slept [68]and ate little. The first thing to attend to was the regulation of a faulty diet, and certain other changes in her mode of living were recommended. A few weeks later I chose the sixth day of menstruation as most favourable in her particular case, and afterwards packed her off to rest and enjoy the sea-breezes alone at Margate.
Within nine months she gave birth to a girl weighing close on 10 lbs. I should add that in both of the above cases I considered as a result of my experience that there was little likelihood of a healthy male pregnancy, and deemed it preferable to make sure of a girl to begin with.
The mother who can bear children early and late and is most prone to male issue is the wide-hipped, deep-chested woman, who has shouldered her share of out-door work or regular exercise, whose digestive organs are unimpaired by rich food, and whose arteries are sound and young even into old age. The little woman who holds herself erect, slight yet agile [69]and well-built, may have a son or two, but the bent-over, “crumpled up,” delicate, nervy, and small-made mother will be far more subject to female issue.
The young girl, who from childhood has been ashamed of her sex-development and who, to look more “boyish,” reduces her hips and chest to a minimum, will never have a healthy and normal motherhood. There are thousands of British girls (and it is in these islands that the species flourish most noticeably) who deliberately try to look mannish, by shoving forward their hips, shoulders and head. With sunken breasts and rounded backs they “slouch” along, mere shadows of what a well-developed woman should be.
Where a surgeon finds “nothing apparently wrong” in a woman who is still young and whose husband is normal, it may mean that everything about her and her way of living is “not quite right.” She may be suffering from habitual constipation and malnutrition. She may simply need good nourishing food [70]in the shape of plentiful fruit, milk, vegetables, eggs, etc., with fresh meat once a day, instead of unwholesome “made dishes,” and rich dainties three times a day.
It is often noticed that fat women are inclined to sterility. They usually imbibe great quantities of liquid, and seem to hanker after thick soups, milk and cream, and all such fattening diet. Their digestion is naturally good, but their nerves are bad, and they suffer from perpetual attacks of extreme exhilaration or depression. Their confinements are difficult and rarely normal, recovery being slow. If they happen to conceive a boy, miscarriages are more than likely to occur.
Another type of woman who is prone to sterility is the lymphatic, lazy and intensely selfish female, who is wrapped up in herself. If she has a child it will be in the early twenties and rarely is the effort repeated.
Sterility may of course occur in both the fat and flabby woman, and the thin and weakly one. The chances of impregnation in both [71]types are encouraged by a healthy mode of living, the avoidance of rich indigestible food, moderation in the consumption of strong tea and coffee, and extreme temperance in the matter of alcohol.
How much ill-health in the married woman is due to the lack of care taken by young girls during their early periods! To be on the safe side, it is often desirable every month to take a day or two off, either in bed or lying on a sofa. This precaution, if made a regular habit, may well help to prolong a woman’s life by ten years or more. In the young girl a little rest at such times might prevent much illness in later years, and add enormously to her chances of child-bearing by giving the virgin organs every opportunity of development without let or hindrance.
On looking into certain cases one often finds that trouble is due to irregularity or prolonged absence of periods, accompanied by a more or less continuous white discharge. Pregnancy is not likely to take place while this is allowed [72]to continue, and it is astonishing how many women suffer it to go on without troubling to effect a cure. When this condition becomes chronic, professional advice is most necessary, and should immediately be resorted to.
A fact which I believe has not hitherto been recorded, but is fully substantiated by my own experience, is that women who habitually suffer from profuse and too frequent periods are more inclined to produce female children, while conversely those women whose periods tend to be scanty and arrive late more generally have male children.
In this connection, I might quote a letter which a lady wrote to me two years ago from India:
I have three little girls and my periods are quite four or five days before the fourth week and always very profuse. I am very anæmic, partly owing to the climate out here. I do so long for a son....
I sent her the advice she requested. Last year she had her wish fulfilled, and, since his birth, the periods are much more normal and [73]rather inclined to be “late” than “early.”
On the other hand I received a letter from another lady saying:
My periods are usually every five or six weeks. Yet I am quite healthy and have never had a miscarriage. I have five sons ... my periods are always rather “late,” but I am very strong and well.
And this leads me to the subject of menstruation, which is generally so closely allied to that of ovulation. In England most girls begin menstruating at 13 years, though large numbers start at 14 or 15, or even later. But according to the record kept by Mr. Robertson of 450 cases, 10 menstruated in their 11th year, 19 in their 12th and 53 in their 13th. He also gives us particulars of great numbers of women menstruating well on to the age of 55, two cases of women doing so till 60, and one of a woman menstruating up to her 70th year.[11]
In cold climates, women frequently menstruate [74]three or four times a year only, and they begin later and end later. In Russia it is not unusual for women to bear children as late as 60, whereas with us it is rare to have a child after 45. Capuron quotes several cases of child-bearing in advanced age. Among these he gives the case of Cornelia, as recorded in Pliny. She was a member of the family of Scipio, and at the age of 60 she bore a son, Volusius Saturinus. Another case he quotes is that of a Venetian physician named Marsa, who treated a woman of 60 for pregnancy, having previously, owing to her age, diagnosed her trouble as dropsy. He adds that a woman in Paris bore a daughter at the age of 63 and nursed it.[12]
It is rare in England to conceive for the first time at 45, but I have known three women who had a first child at 47, and two at 48. Yet so great is the latitude in the ages of women’s fruitful period that a girl may be a mother at 12, or even earlier in hot climates.
[75]
La Motte delivered of a child a girl who had not completed her 13th year, and who had not menstruated.[13] Dr. Paris states that during the year 1816 some girls of 13 were admitted into the Maternité at Paris,[14] and recently the Matron of a London home has given me particulars of two or three cases of mothers of 13 and 14.
Dr. Rowlett, of Kentucky, reports the case of a certain Sally Deweese, born in 1824, who began to menstruate at a year old. At nine years old she became pregnant, and in 1834 gave birth to a female child weighing 7¼ lbs., the mother then being 4 ft. 7 in. in height.[15] It should be noted that in cases where the mother is quite elderly or where she is a mere child, the progeny is rarely healthy or strong. In the former category the child more often suffers from lack of full mental development, and in the latter it rarely survives its birth.
[76]
Having made a brief survey of the question of sterility in women, I may now state my conclusion that most disabilities are remediable, or at least capable of great modification. Much depends on the woman herself—her health, mode of life and temperament. Conditions and the proper choice of a day can help, but where there is some organic or anatomical disability, the advice of a surgeon or a doctor should immediately be sought. In few cases, from my experience, is sterility absolutely hopeless, though in many instances where a girl-child can be conceived, a boy would be impossible, and the attempt should not be made, as it might cause lasting injury to the mother.
I must confess that when the causation of sex loomed large on the horizon of my mind I little thought that the simple natural laws I had discovered would prove such an efficient aid in the treatment of sterility as has since been shown so abundantly to be the case.
[77]
“The sex of the child is fixed before it is fertilised.”—Lenhosick.
Before I go on to describe the simple law of nature on which the pre-determination of sex depends, it is essential that a few anatomical details should be explained and understood. A fundamental truth to be borne in mind is the absolute completeness of the maternal organs. They harbour from the first moment of actual existence the potentialities of both sexes alike, entirely independent of the fertilisation of the male parent. Of what then do the uterine organs consist? Let us first treat of the position of the uterus or womb. This organ begins to develop with the first beginning of menstruation, and it goes on growing until the twenty-first year. Once it has borne [78]a fœtus it never entirely regains its virgin form, but remains slightly enlarged. It lies rather to the right, so that when a woman is on her back, the right ovary and the uterine opening of the right oviduct or Fallopian tube are lower down in the pelvis than the left ovary and oviduct. On either side of the womb are the Fallopian tubes, their average length being four inches. These tubes are dilatable, smaller at the uterine opening and thicker at the abdominal opening near the ovary. Each tube is lined with mucous membranes which, containing special hair-like fibres called “cilia,” impel the ovum, or egg, onwards down the tube by a movement always in one direction, towards the uterus. These tubes are the excretory ducts of the ovaries.
The ovaries grow and mature earlier than the womb. Each ovary is a solid oval-shaped organ more or less encircled by the outer end of its corresponding Fallopian tube, and each enlarges when about to discharge an ovum. The right ovary is larger than the left. In [79]each are a large number of cysts known as ovisacs or “Graafian follicles,” so called after R. de Graaf, a Dutch anatomist, who died in 1673. Each Graafian follicle contains an ovum floating in a clear albuminous fluid, called “liquor folliculi.” At birth there are thousands of ova in the ovaries, but by the time of puberty only one-third remain. Each follicle contains an ovum and each ovum a vital structure called the germinal vesicle or nucleolus. This, when fertilised by the corresponding contribution from the male, grows and develops into the ultimate child.
Ovulation, i.e. the discharge of a ripe ovum from an ovary, is brought about by the development and maturing of a Graafian follicle, its rupture and the discharge of the ovum it contained. The enlarged follicle having gradually approached the ovarian surface, its walls become congested and thinned at one part. It then bursts; the “liquor folliculi” is poured out, and the ripened ovum set free. Ova, one or more at a time, are expelled from [80]the ovary at regular monthly intervals, from puberty to the climacteric, for some 35 years. Before puberty a girl’s ovaries are pearl-grey and smooth, but later each ovulation leaves a little scar. For every monthly period a scar remains, and, as there are some 500 menstrual periods in a woman’s life, there should be in all some 250 scars on each ovary, though most of these are entirely obliterated in the course of time.
As the ovaries are formed in the embryo fœtus so is their sex determined, and they are potentially male or female from the start. The ova, in their thousands, lie latent in each ovary of the female until puberty supervenes. Then, alternately, every month or thereabouts, starting always from the left, each ovary expels its ovum, and does so with increasing regularity as adolescence ripens into womanhood. According to the sex, if at any time the ovum be fertilised and pregnancy ensues, an indelible scar will be left on the one ovary or the other.
[81]
It is only of late years that the theory of the alternate action of the ovaries has been recognised by certain eminent gynæcologists. The evidence afforded by the ovaries themselves admits of little possible doubt as to the fact of equal division of activity between right and left side of the womb. Such action is not simultaneous, but definitely alternating in character.
A woman doctor in Geneva, 35 years ago, made a close study of the fact that young girls frequently complained of pains one month in the right side and the next month in the left. She also pointed out a dissimilarity between the two periods for two months running. These observations combined with others, carried weight in the minds of many prominent doctors, hitherto sceptical of the alternate working of the ovaries, and the theory of “sides.”
To my mind, as the result of long and close investigation, the conclusion is definitely established that the side theory cannot be seriously [82]questioned, and any attempt to overthrow it would result only in putting back the hands of the clock.
Dr. Rumley Dawson’s clearly stated account of the alternate working of the ovaries is too well known to need reiteration in this treatise.[16] It is entirely consistent with the principle, by which as Professor Gamble lately stated, Nature makes provision for all parts of the human body to rest at intervals while other parts are employed, thereby enabling the organs to “work in shifts.”[17] The theory in itself is time-honoured, and many authors can be quoted in support of it. The left side is the first to operate in the young girl, and it is usually the first to push forward the work of conception in the woman. Hence the preponderance of females among all first-born creatures.
In the early stages of life most children are left-handed, they even start walking left foot [83]foremost. As they grow, however, the right side in time takes precedence. The right leg is the strong one to jump from, the right arm wields the weapon with which we work or fight. Similarly the whole right side of the human body is definitely superior in enduring power to the side where beats the heart. In more ways than one must this organ be held responsible for the weaker fibre of the position it dominates.
If there is one exception to this rule it is the brain, of which the left side gets a more rapid supply of blood, and thus shows more activity than the right.
On the other hand in tubercular hip-disease, the left leg is affected in 80 per cent. of cases. Congenital dislocation of the hip is seven times more common in female children than in male. Prenatal and spontaneous amputation of fœtus limbs is usually to be found in girls only. The disaster of being joined together, like the Siamese Twins, is more often suffered by girl-twins, only a very few similar cases among [84]boys being mentioned in medical records at any time. In phthisis, the left lung is the first to be affected in 80 per cent. of all cases recorded. The teeth on the left jaw are the first to arrive, and likewise the first to decay or drop out, with but few exceptions. Again the right hip, leg, foot and hand are almost always larger than the corresponding members of the left side.
So, too, it comes about that the right ovary, the seat of the male ova, is also the more developed, the larger, and the best able to nourish the fertilised embryo. It can afford fuller space and freedom for male offspring than the left ovary can do for the female ova it produces.
As regards the reason why there should be one side for each sex, one might as well inquire why the heart is on the left and the liver on the right. Galen has said that “the right side in both parents produces boys, because it is warmer.” But many people would have judged the side governed by the heart to [85]be the warmest. Be that as it may, the fact remains that in France brides are seriously advised to sleep on the right side if they desire sons, and in 1870 the Lancet observed that “habitual sleeping on the right side produces boys.”
And so we come to my conclusion. With an organism entirely self-contained and independent, as I have endeavoured to show the female anatomy to be, the only reasonable inference is that the male is in no way a determining factor in the sex of the ovum fertilised by him. On woman and woman alone does the sex of the unborn child depend.
[86]
Just as the male ovum proceeds from the larger ovary, so does the development of the male fœtus take place in the larger and more expansive side of the uterus. The male ovary, being more perfectly developed, and more self-contained than the left, throws out its ovum on the third day of the menstrual period, never before. The earliest boy-pregnancy ever recorded started on the third day of the period. It was the notable case reported by Dr. Guérin, of Anne of Austria, wife of Louis XIII of France, who thus conceived her eldest son. Again we are told by Jourdain that Henri II consulted the eminent Fernel as to a means of rendering his Queen Catherine de Medici, [87]fruitful. Fernel advised intercourse “immediately after the period,” and his advice proved successful. After years of disappointment, the Queen gave birth to a son.
My researches convince me, however, that only in rare cases does male conception occur in the early menstrual flow, i.e., from the third day to the sixth day of the period. The greater majority of normal male conceptions occur between the eighth and fifteenth day, counting from the very beginning of the period. The twelfth day is certainly the fruitful day, par excellence, for the conception of male offspring, experience having afforded conclusive proof that the ovum proceeding from the right ovary is then at the height of its receptivity. It must, however, be borne in mind that a boy can only be conceived every alternate month, one month being fruitful and one fruitless. This is further dealt with in a subsequent chapter. In my formula I have always given the fifth day after cessation of the period as the most likely date, allowing a full seven days for [88]the duration of the menstrual period. The reason for allowing seven days to elapse before risking pregnancy is, that, although the actual flow may only last three or four days, the uterus remains in a perturbed state for a whole week, and the ensuing muscular flabbiness is not propitious to really healthy offspring. It is interesting to refer to the Law of the Talmud, which goes to prove that the fourteenth day was largely utilized by the Jews. The direction in Leviticus is “But if she be cleansed of her issue, then shall she number to herself seven days, and after that she shall be clean, and on the eighth day”[18]....
I have known many cases where male-conception occurred on the fifteenth, sixteenth and seventeenth days respectively from the beginning of the period. One happened for certain on the eighteenth day, though this is exceptional. Such belatedness may easily cause a meeting of two ova, as it were, in the so-called “blank week”; one a male ovum and the other [89]a female, which may possibly have been thrown into the tube as early as ten days before menstruation. If these two happen to be fertilised on the same day, or within two days of each other, the result will probably be the conception of mixed twins.
Generally, however, the disappointed ovum, if unfertilised, perishes on or about the fifteenth day, for its life, unlike that of the spermatozoon, is only a matter of days. With the ovum thus dead the uterus is unable, for the next six or eight weeks, to conceive a male child, since, before the next male ovum is due, the fruitless month must elapse.
If, on the other hand, fertilisation takes place, the uterus closes up entirely, jealously guarding the precious ovum that has now become a male embryo. From the first month of conception the embryo is alive, and its sex fully determined. It is an amazing fact that many people still believe that sex can be determined any time after pregnancy until the child quickens. Again and again I have been [90]asked how to change the sex of an unborn infant that was well on its way. People seem to think that a wave of the magic wand, a special diet, or some form of treatment can transform a full-blown girl-embryo into a boy fœtus, or vice versa!
It is equally childish to imagine that the embryo does not enjoy vitality from the first moment of its existence. The virtue which proceeds from the fertilisation of this germ has such prodigious power that the whole being of the woman, in mind and body, undergoes a subtle change. Many women are affected in various ways almost immediately. Some are the victims of nausea and vomiting which last either for the first two or three months, or for the whole time of gestation, and are most distressing and difficult to alleviate. Others suffer acutely from heartburn, cramp, undue salivation, and other disabilities.
As regards the movements of a fœtus, they may be detected by a doctor long before the mother discerns them. Possibly she will not [91]feel them until the fifth month or sixth month of pregnancy, especially if she is of a passive and lymphatic nature. The quickening occurs earlier with boys than with girls. Hippocrates maintained that as a rule the male is felt at three months and the female at four, on account of the greater strength of the male.[19] Dr. Hamilton knew of quickening in the eleventh week.[20] Denman says “quickening may happen from the tenth to the twenty-fifth week, but it occurs most commonly about the sixteenth.”[21] I have found in the majority of cases that with boy-pregnancies it occurs at sixteen weeks and with girl-pregnancies at seventeen or eighteen. “Quickening” is caused by a change in the position of the uterus, which, on account of its increased weight, suddenly rises above the pelvis, thus enabling the movements of the fœtus to be discerned for the first time.
[92]
During the first three months or so the uterus seems to be flatter with a male pregnancy than with a female. This condition prevails up to the time of quickening, when the very opposite occurs. The explanation of this is simple. When the male ovum leaves the ovary and, after the menstrual flow, is fertilised, it finds little or no preparation for its nutriment in the decidua, from which it is to derive its support. Hence its inception is characterised by considerably less spontaneous vitality and development. The female ovum, on the other hand, starts its embryo existence with all the unwasted accumulations of a uterus which has not discharged its contents for three weeks or more. But, as the pregnancy advances, the male embryo makes up for lost time, and thrives apace on the more generous supply of nutrition provided by the larger male ovary.
With advanced male pregnancies, too, there is generally a distinct protuberance on the right side in front. The weight of the fœtus is thrown towards the right, and a characteristic [93]of male-pregnancy is that it allows of a freer walk and less awkward bearing. A lady pregnant with a boy, describes her condition as follows:
I am very large, but it is all in front. I am so nervous lest it should be another girl, but the movements are certainly on the right side.
Another lady who subsequently gave birth to a son, wrote:
I feel all the violent kicking on the right side and I have cramps down my right thigh.
The male sex of a child often tends to cause an extension of the term of gestation beyond its natural limits. This is mainly due in my opinion to the larger size and greater elasticity of the right horn of the uterus, and also to the superior powers of nutriment of the larger ovary. Although quickening occurs earlier in male-pregnancy than female, the movements of the female embryo are generally quicker and less powerful.
[94]
We may certainly conclude that Nature intended women to produce more boys than girls, and that, with this end in view:
1. She provided the girl-child with more male ova in her right organ than female ova in her left.
2. She rendered easier the fertilisation of the right side ovary by placing the right cornu of the uterus, the tube and the ovary, in the more attainable position in the pelvis.
3. She made the right ovary and tube larger than the left and provided more seminal fluid for them to carry.
These facilities for the increase of males are the more necessary and desirable when we consider:
1. The greater tendency to abortion with male-pregnancies.
2. The great care which must be exercised with first children, if they be boys.
3. The lack of proper means for rearing male prematures born under seven months.
4. The extra attention that is always required [95]by boy-children in the way of feeding, warmth, and such necessary treatment as circumcision.
When we have overcome these disabilities, we shall have made a very definite step forward. But even so we shall not be able to obtain a reasonable proportion of males and females until proper use is made of the simple law of determination, with which I have dealt, however imperfectly, in this chapter.
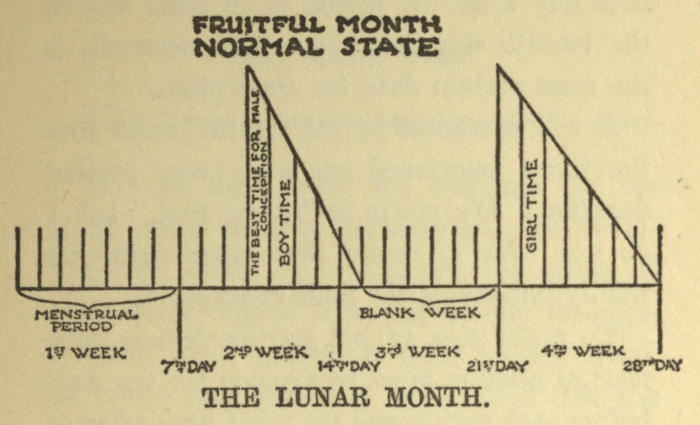
FRUITFUL MONTH NORMAL STATE
Now, for the benefit of the uninitiated and for those unacquainted with medical terms, I [96]intend to make a brief and simple summary of the points outlined, so that any woman who desires to have male issue can make personal use of them.
Union should occur from the third day to the tenth day after cessation of period. The fifth day after the period or in other words, the twelfth day from its commencement, is the most certain date for conception.
It will be noticed by the careful reader that the times mentioned are of a very limited duration. My motto is “safety first,” but I do not wish to imply that other dates are wholly impossible for male conception.
To make sure of not having female issue marital relation must be avoided for ten days before each period and for three days after.
[97]
Having dealt with the workings of the right ovary, perhaps the simplest plan to follow now would be to examine the action of the uterine organs from day to day throughout the lunar month in their proper order. It is not very generally understood that the lunar month of every woman holds a “blank week,” or kind of close-time, during which no conception can occur. Yet this is true of all normal women who function regularly, and the exceptions merely go to prove the rule. Thus, given that the menses be regular, and counting from the first day of the period, a [98]blank week exists from the sixteenth to the twenty-first day of the lunar month.
During that time both ovaries, male and female, are temporarily in a state of apparently complete inactivity. This is what actually happens. In the first week of the lunar month, counting from the period of menstruation, the ovum is discharged. Then follow eight days of expectancy, when fertilisation may have taken place, but after that the womb becomes atrophied, and from that time (i.e. the sixteenth to the twenty-first day) provided she be regular, a woman may safely consider herself immune from fertilisation. If more wives were aware of this fact, many would take advantage of the “immunity” to shield themselves from a too large or too rapid increase of family. In contrast with the drawbacks of so-called “preventive measures,” this is a harmless and innocent means of prevention offered by natural laws.
Unfortunately every woman is not normal, and there are some who may never benefit [99]from a “blank week.” This occurs where the period is habitually too early, often as much as a week or ten days before it is due. In such cases the “blank week” has been trespassed upon, the next period is already on its way, and no respite has been allowed to the harassed uterus. Such indications point to a state of weakness sometimes no more than temporary, and, with proper treatment and care may in time be remedied. But such a condition frequently denotes serious ill-health, such as anæmia, which, if allowed to continue, will cause much trouble. It is also at the root of many abortions.
On the other hand, where the period is retarded for two or three days, or more, the “blank” week may develop into a close-time of ten days or a fortnight. This state of affairs is usually beneficial both to the uterus, and to the general health of the individual. It should, in fact, be stated that the “late” period is a sign of strength, and as long as it is not attended by any other troubles, or by [100]distressing “white discharges” in between the periods, should cause no kind of anxiety. Most healthy young girls are “late” for many years after menstruation begins, and sometimes go on for four months without a period. These girls I have found to be quite healthy and normal, enjoying easy confinements in married life, in contrast to those who are perpetually troubled by “early” or even “regular to the day” courses and by an over-profuse catamenial flow.
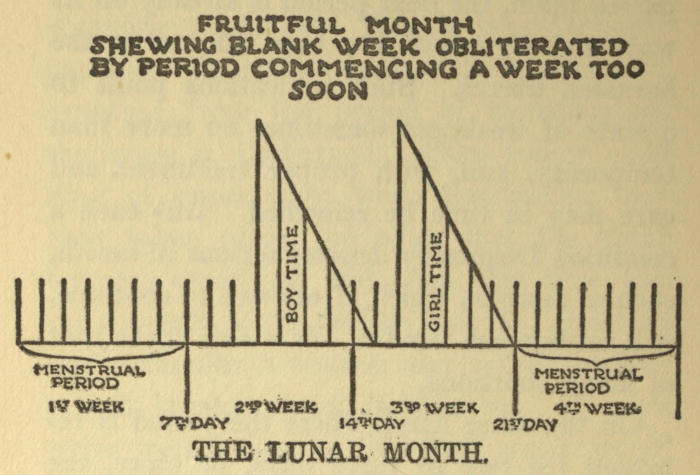
FRUITFUL MONTH SHEWING BLANK WEEK OBLITERATED BY PERIOD COMMENCING A WEEK TOO SOON
[101]
It is the latter class of women who are far more susceptible to the fertilisation of the female ova. With persons of rarer and “late” periods, the very opposite conditions prevail. To take a few instances, a woman I know had but one day of actual “flow” every six weeks and invariably relied on a “blank” of twenty days. She gave birth to seven boys, but not a single daughter. Again a certain French peasant woman only had a day’s period every two months; her family consisted of three boys and no girls. An American lady, who gave birth to eight sons and one girl, had a period regularly every five weeks, lasting half a day only. Her first-born was the girl, and it was remarkable that, in early married life, she had been more “regular” with scanty periods.
A lady wanting a son wrote to me as follows:
I fear my periods are very irregular—always three weeks late. I have never had a mishap and am very healthy and robust.
[102]
She had two boys in succession.
Another wrote:
I am very regular, but invariably “late,” 32 days being the usual time.
She had sons only.
Another letter runs thus:
Before the birth of my girl I was always very regular at 28 days; now somehow I am always “late.”
Her three following children were boys.
I could give innumerable cases in further support of this contention. In a like manner my available evidence goes to prove the tendency to girl-pregnancies among women of profuse and “early” periods. This is readily understood, when one considers how easily the “blank” week may cease to exist, obliterated by the over-active left ovary, so that the unfortunate wife becomes the mother of an unlooked-for girl. Every alternate month the danger is present, and, though often avoided, [103]may sooner or later cause the advent of a daughter.
A lady writes thus:
My periods are very profuse and always too early; I long for a son, but have had only four girls.
Another writes:
I never have more than ten days entirely free ... but my confinements have been quite normal ... I have two little girls.
With the women of rare and scant menstruation, on the other hand, the “blank” week is very real and reliable.
Lady A. wrote to me as follows:
What you tell me about the blank week I have heard discussed, and some of my friends make use of it.... Twenty years ago, Lady E., a very old friend of mine, said to me in private: “Now, my dear, I do wish you would warn my niece not to have any more children. She is shocked at the idea of preventives, but were you to tell her all about the ‘blank week,’ as my mother told me, I am sure she would make full use of it.”
[104]
The mere fact of the right ovary remaining quiescent till its appointed time proves that the male ovary is probably the healthiest and the most likely to produce ova for fertilisation. The right ovary unless diseased is never too early. This is chiefly due to its being naturally stronger and more self-contained, and discharging its ovum after the period has actually begun. Where the periods are too early, it will be generally found that one ovary works quicker than the other, and that this ovary is the left.
Thus it is possible for three weeks to elapse after one period, four after the next or two weeks one time, three and a half the next and so on. If it happens that the male ovary is also “early,” after years of irregularity, this is because of a “reflex” activity, resulting from the insistent stimulus of the left side.
Generally speaking, just as a tendency to constipation bespeaks in any given person better health than proneness to diarrhœa, so the longer “blank” week and the “later” period [105]prove more strength in a woman than the “early” and profuse menstruation. The latter trouble needs drastic treatment; the former responds to gentle coaxing and modifying.
Having thus shown the existence of a “blank” week, which provides immunity from conception to every female enjoying normal health and regular menstruation, we now arrive at the twenty-first day of a woman’s lunar month. Adhering to my programme, let us proceed to examine what occurs, in every normal woman, after the completion of the third week of this fruitful month.
I hope my readers will be clear in their minds, in so far as we have arrived at the point already demonstrated.
(1) When male children are safely and easily begotten.
(2) When the blank week affords nature’s means of repose to the organs of procreation.
[106]
On the twenty-first day of a woman’s lunar month a change occurs in the uterus. Activity commencing in the left ovary affects the whole being in a greater or lesser degree. Slight pains are experienced in the back, and the sensitive and highly strung feel a tenderness in the left breast and left thigh, as in the same way during the next month such pains may be felt on the right side. The left ovary has become restive, and, already seven days, and sometimes nine, before her “flow” is due, has ruptured the Graafian follicle, setting free the female ovum. This premature rupture of the vesicle, with the bursting of the Graafian follicle, [107]is brought about by the actual formation of the “female” ovary, and, its development being less than and its retentive qualities inferior to those of the right side, the female ovum is often launched as much as nine days before its menstrual flow is due. The life of this ovum, like that of all ova, is from eight to fifteen days, and, in a normal woman, it is receptive to fertilisation from the twenty-first to the twenty-eight day of the lunar month which terminates with the next period.
Thus in all normal cases, the twenty-first day of the lunar month, or the seventh day before the next period is the most likely day for conception of the female offspring. Healthy and regular cases are in a large majority; indeed, among native women, untouched by modern civilisation, they are probably the general rule.
A lady writes:
I have three little girls ... and they were all started before the period.... I seem never to be able to conceive at any other time.
[108]
Another says:
I was told that boys were conceived seven days before the period. I tried this method, but it was a girl.
Herein lies the true explanation of the fact that nearly all first children, who are not “prematures,” and born within the first nine and a half months of marriage, are girls. The bride generally arranges that her wedding shall take place the second week, after the period is safely over. She thus carefully selects for her marriage a date, at least ten days after the expiration of menstruation; which, if it happens to be the fruitful month, will fall in with the girl-conception time. And, if she conceives, her first child is bound to be a girl.
In order to make sure of my ground, and in deference to the expressed wishes of many gynæcologists, I have taken statistics relating to this over a number of years, running into a thousand cases, with the result that 80 per cent. confirm my dicta—than which there could [109]hardly be better proof. If to these statistics is added the fact of the greater activity of the left ovary in young womanhood, I submit that the combination of conditions renders my statement of the facts almost irrefutable.
There are many women who can only conceive a girl on the last three days before the period is due, showing that in their case the ovum is discharged shortly before the flow starts. Other women again are unable to conceive at any time except on the very day the period is actually due—I know of many such; they all had girls and never a son. But in all these cases I have found a certain morbidity of the uterine condition, combined with a tendency to hysteria and nervous disorders.
The closely impending flow, though not yet present, must render the existence of the germ precarious, and is usually conducive to bearing-down sensations at the menstrual times. This is often accompanied by a slight “show,” which may cause alarm, though not necessarily in any way a serious matter.
[110]
Here let me state most definitely for the benefit of those mothers who desire female issue, that the great majority of girl-infants are conceived on the seventh or eighth day before the period is due, those being by far the most actively receptive days for female pregnancies. It is the seventh day that I have always advocated in my formula, and on that day, in all normal cases, the strongest girl-babies are conceived.
It must be remembered by those wishing to profit by my formula that a girl can be conceived only every alternate month, one month being fruitful and one fruitless.
It is not difficult to find out which month is fruitful, but it is perhaps wiser to avoid confusing the issue by making calculations with regard to this contingency.
In order to avoid male issue relations must not take place for ten days after each period.
[111]
Those readers who have followed the argument so far will have gathered from the last chapter the nature of my claim that every normal and healthy woman is able to conceive a girl according to the method indicated. But it is now necessary to touch on the small percentage of women coming under a different category.
It must be repeated that the normal state of every woman is to have one fruitful month followed by one fruitless. The fruitless month affords occasion for conception of both sexes, whereas I am satisfied from the investigation of a very large number of cases that complete immunity from pregnancy exists every other month. These quiescent weeks can easily be [112]discerned by any normal woman, who experiences during that period a sense of partial lack of sexual activity. Thus, out of every eight weeks, the functions have five week’s respite, which affords the recuperative advantages demanded by nature. And so just as there is a blank or fruitless week in the fruitful month, so there is also a fruitless month in alternation with the fruitful one.
And now we have to discuss a condition of the left ovary which may result in conception taking place during the earlier days of the fruitless month. I refer to the freak action of the “left” ovary. Much confusion of thought and biological error have been caused by this condition, the result of an over-strained civilisation and the increasing artificiality of our mode of life.
In some women, and for some unexplained reason, the left ovary takes upon itself an added activity equal to that of the right ovary, while at the same time the functions of the latter decline until finally it ceases to contribute [113]anything to the reproduction-life of the woman. The left ovary, having acquired so much importance, becomes, as it were, unbalanced with the weight of its responsibilities and runs amok. The ovum is discharged about the twenty-first day, as we have explained before, but instead of dying as the result of non-impregnation, it actually remains in the womb and lives during the whole time of the succeeding period and may even live for several days after this is over. Thus there is now the risk of the ovum becoming fertilised during the early days of a fruitless month, and this state of affairs is entirely due to the condition I have called a “freak” ovary.
Such an activity, foreign to its natural state, may be temporary or lasting according to its subsequent functional history. The result of such investigations as have been made appear to show that among natives of comparatively uncivilised lands, this action of the so-called “freak” ovary is practically non-existent—all the evidence obtainable points to [114]their immunity from the effects of such ovarian breaches of the usual procedure have come to my notice.
And now we are negotiating the rock on which so many enquirers have foundered whilst seeking the causation of sex. The existence of the “freak” ovary has apparently exploded the simple formula of “Boys after, girls before.” The formula would have held good but for the fact of the freak ovary being too common to be overlooked. The vitality of this ovum interfering with the so-called “fruitless month,” in which every normal woman is safe from conception, is most disturbing, and, in the early years of my work, this abnormality caused me much trouble. Now that I have solved the problem I regard this factor as the corner-stone upon which rests the whole structure of my discovery.
Subtle and yet so definite when revealed, the distinct operations of each ovary have given me the key to the explanation of a very baffling question. The month in the ordinary course [115]should be fruitless, because, had the left ovary menstruated and thrown out its ovum seven days or more before the flow, it would by the actual day of the period have lost its vitality, and, if unfertilised, been carried off by the flow itself. In its turn the right ovary, when due to menstruate, would leave quiescent the uterus until the actual moment of the period, and discharge its ovum after the third day of the flow, or even later.
With the presence of the “freak” ovary, however, all this is changed. We find the ovum still active and dangerously receptive on the second and third day after cessation of the menses. And so the girl-child, which is conceived after the period (although in a different month to that of the boy) suffices to undermine the old adage, “Girls before, boys after.” It is, no doubt, this anomaly which explains, to a large extent, the utter lack of practical conclusions reached on this question during past centuries of biological thought. The vast numbers of test-cases collected during the last [116]twenty years, and proved to the hilt, entirely dispose of the idea that boys only can be conceived after a period.
But it so happens that girls, if conceived after a period, generally start during the so-called “fruitless” month. Innumerable cases may be cited of girls conceived on the fifth and sixth, seventh and eighth day of period. This is much to be regretted, for it is easy to see that an ovum fertilised during the actual flow of a menstrual period has not the best chance of growing and developing into a healthy infant. The womb is in a perturbed state, and its lining hardly offers a suitable bed on which the delicate ovum can rest.
The Old Testament has warned us sufficiently against this evil.[22] Abortions are liable in the early months of pregnancy, and everywhere we see the results of such intercourse. Many women with skin troubles, blotches, or marked with the ugly “port-wine stain,” or nævus spot, are examples of relations at this [117]period. To every hundred women thus disfigured you will find scarcely one man. Another result of this unwise intercourse is a large number of big moles all over the face, especially on the left side. The fact that this condition is rarely found in men shows that the conception of boys during actual period is very rare, if not almost unknown. The earliest date recorded of boy-conception is the third evening of period. The seventh day is the earliest date probable after menstruation, counting from the first day.
When one realises that conception at the menstrual period is actually due to a morbid condition of the uterus, dependent on a slightly abnormal ovary, one can gauge the undesirability of risking the advent of such offspring. Indeed, it is important that the self-respecting mother should see that no child of hers be tainted with the reproach of the premature intercourse above described.
If girls are conceived in the first three days after period (during the sixth, seventh, eighth [118]days), that is another matter: they may be the healthy offspring of a slightly abnormal mother who generally can only conceive at that one time. For instance, Lady D. writes:
I can never start a baby at any time except immediately after my period. It is always “early” and too profuse.... I have three girls, and do not seem able to have a boy.
It should, however, be understood clearly that no woman, in a normal healthy state, conceives girls in the “fruitless month.” Invariably all the cases observed of this nature occur among women suffering from the results either of a severe boy-confinement, or an abortion which has seriously affected the male ovary and left it in a diseased state. Again it may happen where the right ovary is naturally weak or has been injured in early youth. From India, a lady writes:
I have a little girl ... but I had several miscarriages before she arrived, from which I have never rightly recovered. It was partly the climate, and also I did far too much....
[119]
Mrs. B. wrote to me from East Africa:
I shall be forty next birthday. My first was a girl, then came a boy born at six months, who only lived a few hours, and I was desperately ill. Then came three girls in succession.
With regard to the offspring of the freak ovary, there certainly seems to result a less healthy pregnancy all the way through, a more difficult and generally premature confinement, and a smaller and weaker infant. I should add, however, for the comfort of mothers, that these children, given suitable environment, often grow up to be as fine and healthy as those generated from a more normal ovary.
It is only right to acknowledge that, in the researches which have enabled me to fathom the complex problem of the “freak” ovary, my best friend has often proved to be my sex. It takes a thief to catch a thief—it required the intuitive brain of a woman to understand another woman, and to investigate with success the most capricious of her organs.
[120]
“Lie on the right for a boy, on the left for a girl.”—Albertus Magnus.
Whenever I am asked to provide a formula for the benefit of those seeking advice on the subject of pre-determination, I have always expressed the opinion that a slight inclination to the right, during and after intercourse, is helpful to the conception of boys, and vice versa for girls. No doubt this flavours of an “old wives’ tale,” and is not new to many married folk. Indeed, it was known as far back as 1582, when Albertus Magnus gave his support to the theory, which subsequently remained a more or less popular idea. At the same time, it is interesting to note that anatomy supports this time-honoured theory in [121]every way. Stock-breeders still make use of it when they place a mare or cow on ground sloping away from the side they wish fertilised. But it succeeds only when they happen to fall on the month suitable to the discharge of the ovum desired.
When I touch on the relation of animals to my theme I do not mean to imply that they function on parallel lines to women, as regarding the alternate month. It is true that the principal laws of nature apply to them in similar fashion, but in this case there is a distinct difference. A certain veterinary surgeon was, in a hundred cases, successful in the use of “side-sloping” with cattle, but the lack of further knowledge concerning times and dates produced the small number of exceptions which acted as a deterrent to renewed efforts in this direction. And yet there should really be no difficulty as to times and dates, the only problem being to select the male month or the female.
Thus a heifer should be watched from the [122]time of the first “rut,” which means the activity of the left ovary. Her times, right and left, should be systematically noted from then on, until she goes to the bull. If the first calf be a heifer, the next heat will accompany activity of the right ovary. A month should be skipped (a good thing in itself for the vitality of her next progeny) and the following heat fertilised if another heifer is required. A well-known doctor in South Africa made observations on a cow he owned in 1897 which had a bull-calf at foot; she had a heifer-calf the next year. He then tried the experiment of missing the next rut—that is twenty-one days after the birth of the heifer, by keeping the cow stalled for a month. She was then allowed to mate, with the result that the next calf was a heifer. He repeated this three times in succession, each time obtaining a heifer. To prove that the cow was normal he allowed her to mate within three weeks of the birth of the last heifer and she gave a bull-calf. This satisfied him that sex can be regulated at will, and that [123]the whole question lies within the functions of the female. That is just one clear case in point, but innumerable similar successes have been recorded by others who have experimented on these lines. The differences of the organic functions of a mare or cow explain why there can be no question of “before or after,” as in the case of women. But one thing I have observed, and that is the importance of taking advantage of the early “heat” to ensure success for a heifer, while the later “heat,” or the second day of the “heat” is more suitable for a male pregnancy.
With regard to the position of the fœtus in the cow, there is a marked difference according to the sex of the fœtus. If heavy with bull-calf, she will usually lie on her right side; similarly it will be noticed that the weight and movements are much more to the right and the side will be most inclined to hang. With female progeny the conditions are reversed. The left side is now the largest and heaviest, and the cow will lie on it most readily.
[124]
In animals producing numerous offspring each time, such as cats, rabbits, etc., both ovaries function simultaneously. The spermatozoa must run equally into both sides of their uterus, for the reason that it is not a simple cavity, but divided by a deep cleft into two parts with a corresponding projection inside the cavity. Therefore, as cats and rabbits have litters of mixed sexes, it is impossible to draw inference beforehand as to their condition.
Then, just as two conditions, time and position, are necessary for the successful fertilisation of cattle, so must the three following conditions be accepted by women, if the results are to be what they desire:
1. The fruitful month must be assured. This cannot be foretold until after the birth of the first child, but it is of little importance compared with the second and third conditions.
2. The day, in the fruitful month, proper to the sex desired must be carefully chosen.
[125]
3. The inclination to right or left, which assists access of the seminal fluid to the male or female Fallopian tube must be observed.
Among all the theories for sex-determination advanced of late years, that concerning Lateral Decubitus is the best supported by evidence. Dr. R. von Braun discovered the earliest evidence of pregnancy in a furrow which forms and divides the uterus into two lateral halves differing in shape, the pregnant half and the non-pregnant. Montgomery speaks of a “boy conceived after the period” and lying “in the right iliac region,” whose mother had complained of muscular pains “round the right Fallopian tube.” Dr. Tuckey, on several occasions, found that the position of the placenta, (the vascular bed to which the fœtus is attached and through which it is nourished) differed according to the sex of the fœtus. It was, in many instances, attached to the left side of the mid-line when the child was a girl, to the right when it was a boy, Montgomery [126]mentions also that a “female fœtus is turned towards the left side.” There is much evidence to show that a girl fœtus is always carried in this position, while the boy faces to the right. Hence the movements are felt towards the left with a girl and towards the right with a boy.
It may often be observed that a woman starting a female pregnancy is quite unconsciously inclined to hold her left side, as if experiencing a slight discomfort. With her, the first movements of the child will be felt in the left groin, while in a boy-pregnancy the opposite will be the case. I have by me a letter from a Mrs. B., which runs as follows:
I had a very bad pain on the left side, when my last girl was born. My periods are always early now.
Mrs. M. writes:
I have had four sons ... in carrying the last two I used to get severe pains in my right groin, caused, I was told, by pressure.
[127]
Lady R. writes:
I always lie on my right side: in fact, I feel comfortable in no other position.
She had three sons.
I have frequently been able to diagnose the sex of the child as early as nine weeks after conception, by the presence of a small round protuberance which appears high in the left groin if a girl, lower down to the right side if a boy. In a fair number of cases I have found the fœtus lying so much to one side or the other that the opposite side appears to be filled only with a fluid, so soft and elastic is it compared to the other. When this condition prevails one can foretell the sex with unerring certainty. The woman pregnant of a male child, according to French authorities, walks right foot foremost, and the right breast will be harder and larger than the left. These differences, of course, are not so discernible in some women as in others.
In the matter of symptoms there is a distinct dissimilarity between boy and girl-pregnancies, [128]which also goes to prove the theory of right or left sides. For instance a woman with male pregnancy will complain of cramp down the right leg, and of soreness in the right breast. The reverse will be found in girl-pregnancy. Less sickness is experienced in boy-pregnancies, and there the mother suffers much less from the presence of distressing “whites.” Many women suffer from the latter to a most troublesome degree when carrying a girl, although with their male pregnancies they experience nothing of the kind.
The movements of a male fœtus are stronger, heavier, and slower than in the opposite sex, and so also is the pulsation of the placenta. It is easier to locate the heart-beat of the male than the female fœtus. It can generally be located by the use of a stethoscope, and if it be a male fœtus, the beats will be low down in the right groin: or if the position be sessile (one in which the breech is presenting) the heart-beat will be high up on the right side. With a girl the beats will be heard [129]either low on the left side or towards the mid-line, and if sessile, high up on the left side. In any case they are always more difficult to discern, as the girl lies to the left with the heart turned away from the surface of the womb. In certain cases the heart-beats of the female fœtus have been heard on the right side, especially where the child has been extremely lively and restless. But it may safely be said that, in nearly every case where this has been noted, the mother was suffering from a kind of semi-sterility, where the uterus appeared to be governed wholly by the left ovary, which in such cases assimilates the characteristics of the right ovary, and thus the woman is sterile in regard to one sex.
It should be remembered of course that the uterus naturally inclines to the right, and in some cases the attraction to the left, noticeable in a female pregnancy, does not take place spontaneously. Especially will this be so if there be a strong adhesion binding the womb to the right ovary. Such adhesions often bring [130]about a disability of that ovary, although the fœtal position may appear, falsely, to indicate a male pregnancy.
It must be here pointed out, that, as a general rule, it is rather the exceptional and abnormal cases that are brought to a doctor’s notice, and seldom those that are healthy or normal. This, no doubt, fully explains why so often medical men have been led to make their deductions from evidence quite contrary to that to be found, if looked for, in the great majority of normal cases.
When all is said and done then, it may be safely concluded that for useful purposes Lateral Decubitus, though not, perhaps, a potent factor, may prove of use in the pre-determination of sex. It is certainly a popular theory, and so far no evidence has been adduced sufficient to disprove its relative efficacy, while some support can be gained from the facts of female anatomy. I have given it in my formula for many years, and so far have never had it disputed, or even questioned.
[131]
I have already in a previous chapter remarked upon the noticeable differences which arise between male and female pregnancy.
A boy may possibly cause a difficult first confinement not only because he comes into the world with a larger head, but also because his average weight is one pound more than that of a girl. It is some compensation to know that the after-effects of a boy-confinement frequently prove more pleasant and straightforward than those which attend upon the birth of a girl.
[132]
It is often said that the majority of still-born babies are boys, though this has never been fully proved, probably because so many still-born illegitimates are not registered; my own experience is rather to the contrary. “Placenta prævia” more often occurs with female issue, and it is generally due to the fertilised ovum embedding itself in the anterior or posterior wall of the uterus near the cervix. It may be that the position of the left ovary, which is on a higher level in the pelvis during intercourse, accounts for this frequent aberration of the ova.
Phlebitis, or inflammation of the veins, is likewise a more common complaint with girl-confinements. It is explained by the fact that any activity on this side more directly affects the functions of the heart. After the advent of a girl-baby, obstinate backache and symptoms of depression are also frequently noticeable, owing to the weaker ovary having greater difficulty in the healing of the corpus luteum and in the control of its own more obstinate [133]discharge. Attention is called to this by the provision in Leviticus “If a woman have conceived seed, and borne a man-child, then she shall be unclean seven days ... she shall then continue in the blood of her purifying three and thirty days ... but if she bear a maid-child, then she shall be unclean two weeks ... she shall continue in the blood of her purifying three score and six days.”[23] The Jews thus made allowance for the discharge lasting twice as many days after the birth of a female child as after the birth of a male.
There is no doubt whatever, that, even if the left ovary is not rendered hors de combat more easily than the right, it will always give the maximum of trouble on the smallest pretext. During pregnancy there may sometimes be a slight “show” at the ninth week, and sometimes after, which, though generally fairly trifling, is sufficient to be alarming. With a boy-pregnancy this may occur in the fifth week, but should it happen later on, it would mean a [134]mishap. With a girl-pregnancy, however, it may often happen, and does not necessarily impede the satisfactory development of the female fœtus. Brierre de Boismont states that out of 1,200 cases, eight showed menstruation during the second, third and fourth months after conception, three showed menstruation occurring throughout the whole period of pregnancy, and one was the case of a woman who menstruated throughout her eight pregnancies.[24] Dr. Nicholson, writing from St. John’s Island, says: “A regular monthly discharge during pregnancy is not an infrequent occurrence in this island, particularly with the whites of a sanguine temperament.”[25] It would be safe to say that the result of such an anomaly would be the birth of a girl, for I do not know of a single case of a boy living longer than a few days, or possibly weeks, after such a gestation.
The first sure symptom of parturition with [135]a female child is generally a “show.” In the case of male issue, in normal circumstances, this is rarely observed until after the waters are discharged. In fact, in practically 80 per cent. of all cases, the parturition of boys begins with the breaking of the waters. A similar proportion of girls herald their advent with a slimy mucus followed by red discharge. These facts go far to confirm the old French saying that “the sanguine temperament begets boys, and the lymphatic begets girls.” It may be that the male child assimilates more red globules and sanguineous tissue in its composition, whilst the female feeds readily on the lymphus and white particles of blood nutriment.
As time goes on experience teaches that the condition of the blood when a girl is carried has different characteristics from those in a male pregnancy. The quantity of fat and albumen is rather increased in the former and the proportion of fibrin and hæmatoglobulin possibly greater in the later. Certain deductions, [136]as to these points of difference, have been gathered by the presence of fatty tissue all over the body affecting even the finger tips during pregnancy of a female child, whilst the contrary condition exists in the state of male pregnancy.
“Flooding” is more frequent after the birth of a girl than that of a boy, and the wearisome symptoms of over-profuse menstruation, appearing for months or even years after childbirth, are infinitely more persistent when a girl-baby has produced the weakness. Again, the displacement of the womb, and its inability to return to its normal size after confinement, is a distressing trouble due to the greater inherent weakness of the left side.
It is important to bear in mind that many unhealthy and delicate mothers would miscarry with a male fœtus whilst a girl-pregnancy might go full time.
As regards the actual labour, the first pangs, with a female child, are more apparent in the back and left groin, and the advent of the discharge [137]soon makes the mother willing to lie up. With a boy, however, the pains are more apt to be felt in the stomach and down the right thigh, and it is easier to keep up and about until the last moments. A curious anomaly is that “after pains,” generally supposed to be unknown at a first birth, are frequently present in first girl confinements. I have not heard of a single instance where “after pains” accompanied the birth of a first child who was a boy. In a tedious labour, it is the first stages that are lingering and difficult with a girl, with a boy the latter stages are the worst.
One cannot sufficiently reiterate to all young women the criminal idiocy of attempted abortion. As a result of my clinical experience I have come to the most definite conclusion that the right ovary, lying as it does lower down in the pelvis, is the most easily damaged. Any adverse conditions affecting the womb may interfere seriously with its functions; such an occurrence as bleeding, as the result of an abortion, may so react on the right ovary and the [138]Fallopian tube as to paralyse them and prevent all subsequent activity.
Where this occurs the left ovary straightaway takes upon itself the functions of both and with redoubled activity, discharges its ova, “capturing the trade” of its rival, so to speak. As we have seen, this ovary produces only female ova; so, henceforth, as a natural consequence, only female offspring will be produced by the damaged womb.
After a first fatal abortion, whether accidental or voluntary, too often a trail of girls will ensue, and I could tell of countless such instances. A lady, pregnant of her first child, slipped downstairs; as a result she gave birth to a still-born boy; the next six children were all girls. I know of another case where eleven daughters followed the premature advent of a male child. In yet another case sheer folly brought about the miscarriage at first pregnancy of a male fœtus; only after many years was the woman in question able to give birth to three children—all girls. In each of the above [139]instances the birth of an heir was of the utmost importance in view of title or estates.
A lady who had given birth to seven daughters had subsequently five mishaps, each at four months, and every time she proved to have been pregnant of a male. Another lady consulted me, because after eight girls, she longed for a son; she became pregnant but miscarried at four months of a boy. I learnt that she had had two similar mishaps before her daughters were born.
It is safe to say that 80 per cent. of all miscarriages are the result of male pregnancies. I am able to give such a figure and to be positive as to its accuracy in my own wide experience, because of the possibility of diagnosing the sex of a fœtus at a very early stage. A striking demonstration of what can be done in this direction was given by Nagel, who distinguished a testicle in the youngest embryo ever successfully analysed with reference to sex; it was exactly five weeks old. And any abortion younger than that does not need to [140]be considered in relation to sex determination.
All women then should be warned early in married life against any risk of miscarriage, that they may be on their guard against such deplorable results, the bane of motherhood. “Fore-warned is fore-armed,” and a huge percentage of the waste of life and energy which now prevails could be prevented if only a more sensible and normal view could be taken on the question of initiating young girls and women into the wonderful, yet simple, laws of maternity, on which all human welfare depends.
[141]
“Conception may take place even though there coexisted an immense amount of disease in the ovaries, provided one of them retained as much of one ovary sound as belongs to one mature vesicle.”—Morgani.
There are and always have been so many dissentient opinions on the vital question of sex-predetermination, that it would be well to survey the multiple causes of the scepticism hitherto expressed by some biologists at the mere mention of the “Side-Theory,” since this theory forms an integral part of my principle.
The root of my argument lies in the statement that the right side contains male ova only, and the left side female. I have examined the “Side-Theory” from all points of view and studied the history of its origin from every source at my command. To satisfy the judicial [142]and unbiassed mind, one must hear each argument and then methodically endeavour to answer one by one with irrefutable proof and evidence; only so can the truth of the theory be established, and the weakness or irrelevance of the criticisms advanced against it demonstrated. It is not an uncommon thing for a woman, for one cause or another, to have one or both of her ovaries removed.
I have gathered many instances of this, and it may be said definitely that no woman who has ever had her right ovary and tube completely removed, has ever given birth to a boy subsequently; and similarly after removal of the left ovary and tube the birth of a girl is not possible.
A few critics have written to me from various parts of the world intimating a knowledge of cases where the right ovary had been removed, and yet a boy had been born, and vice versa, drawing the conclusion that such evidence entirely disposes of my theory.
My reply to them is that I can go further, [143]as I know not only of instances such as they draw my attention to, but others in which both ovaries have been removed, and yet children of both sexes have since been born. The explanation is perfectly simple. It sometimes happens that if the operation is not absolutely complete, a vestige of pedicle stump remains sufficient to harbour one mature vesicle, and that being so, pregnancy undoubtedly becomes possible.
Some time ago a rising young surgeon expressed the wish that he might come across one single case of a woman bearing a child, after both ovaries had been removed. Then only, he said, would he be prepared to “accept the theory of sides in its entirety.” Shortly afterwards he was able to realise his ambition. A medical friend of his delivered of twins of differing sex a woman who had actually been operated upon by that same surgeon a year or two previously, when both ovaries had been removed. From medical authorities I have been able to gather a few more such cases, to [144]add to my own list. And it is only recently that a lady wrote to me: “I had both ovaries removed and tubes, but since then have given birth to a boy and a girl.”
Experiments on animals, after the removal of both ovaries, go to prove that they may still produce young, just as cases are recorded of certain male animals being able to fertilise a single time after being castrated, and the explanation is simple. In ovariotomy it is sometimes difficult to ascertain that all ovarian tissue has been completely removed. Some of the tissue may yet remain in the pedicle stump, and if this pedicle stump be long, one cannot say how far up the ovarian tissue may extend.
Montgomery gives a case of boy and girl twins born in such circumstances. In the postmortem on the mother only one corpus luteum was discovered, the left ovary having been removed. The pedicle stump, had, however, harboured the female Graafian follicle; hence the girl. On the right ovary, the single corpus luteum could not possibly have contained the [145]two Graafian follicles necessary for the embryo of each sex. A lady I knew of, who had her right ovary removed, became pregnant two years later; about the third or fourth month she was taken very ill with pains in her right side and intense hemorrhage. The doctor advised an immediate operation for tubal pregnancy; this, however, was not eventually found necessary, as the trouble subsided, with the discharge of a blighted fœtus. Later, the patient was assured that this side would be of no further use to her, as the tube “had evidently burst”; thus precluding any hope of future offspring; this diagnosis proved wrong, because she has since then given birth to two sons.
Twins may arise from the same follicle, but they will be of the same sex.
Menstruation may continue after both ovaries have been removed, and invariably does so where only one has been removed. But the fact of so many women being able to conceive after bi-lateral ovariotomy, and to conceive twins of either sex, when only one corpus [146]luteum has been found in either pedicle stump, proves to the hilt the truth of the “side-theory.”
Another striking testimony to the law of sides is afforded by tubal or uterine pregnancy. This unfortunate condition is caused by the ovum being arrested in its passage from the ovary into the uterus, and so being fertilised while yet in the tube. A morbid state of the tube, which has possibly formed adhesion with the ovary or other parts, may be due to congestion or contraction of its natural diameter. This practically never occurs except where previous children have been born and is most common where there has been abnormal distension, such as an unusually big child or twins might cause. Death may ensue from the bursting of the tube, and the results of many post-mortems on such cases have added their testimony to the correctness of my theory.
Male tubal-pregnancies are the most usual, since the right tube is the largest. Dr. Seligsen of Moscow collected fourteen cases of [147]males in the right tube; of females developing in the left I have collected five. In one case, where a female fœtus was found in the left tube, which was removed, the mother recovered and had a boy four years later. Of the right tube I have collected six cases. In two the mother recovered without the tube having to be removed, the fœtus coming away at four months after acute pain in the right side. If, however, the pregnancy lasts for over sixteen weeks the tube invariably bursts, unless otherwise relieved.
In another case the right tube, without bursting, ejected the cigar-shaped male fœtus at four months, after severe hemorrhage. The patient recovered, but two months later a second male fœtus was ejected from the uterus, and severe ovaritis ensued. This was cured and the woman became pregnant again of another male fœtus which aborted at two and a half months. The ovaritis reappeared, whereupon an operation was performed, and the appendix was found to be adhering to and [148]pressing against the ovary. After the removal of the appendix, the ovary promptly recovered its normal health. The original cause of this trouble had been the abnormal size of twin-boys, born some two years previously.
A girl under my observation had to have her left ovary removed, before she grew up, as the result of a severe accident; later on she married, and gave birth to six boys in succession. Another girl who also had lost a left ovary married and gave birth to a boy and then to twin-boys; since then, she has had two male miscarriages at four months; neither of these women ever had female issue.
A girl who strained herself at thirteen playing tennis, complained ever after of pains in the left groin; she married and has given birth to seven boys in fifteen years; evidently her left ovary had been rendered inoperative. Numerous instances of this kind could be given, and every case I have come across has emphatically endorsed the side-theory.
No doubt there are occurrences which seem [149]to tell in the opposite direction. For example a male fœtus may be found growing in and distending the tube leading to the womb from the left ovary. But this can be explained quite naturally by the fact that the male ovum had journeyed from the right ovary, down the right tube into the womb, and then, instead of remaining there, had passed right across the cavity into the left tube; here it had become lodged, and so developed into a male fœtus; this is called “internal migration.” Or again it may by “external migration” have passed across the pelvis cavity, along the peritoneal surface of the intestines, to the external opening of the opposite tube—the left.
This, however, savours of an accident, and in no way disproves my theory that the right ovary produces male offspring, and the left female only. Experts have mentioned both these anomalies, but have so far offered no explanation, though Pouchet advanced the doctrine that there might be, in these cases, “aberration in the dispersion of the semen [150]which does not follow its natural course,” of which no proof is even suggested.
Professor Scanzoni cites the case of a woman who after a quarrel with her husband, complained of severe pains in her left side and died that night. On examination a laceration was found on the left side of the uterus, in which were the membranes and placenta of a fœtus, but there was every evidence that the ovum had originated from the right ovary.[26]
A Mrs. C., after the birth of two girls, employed my formula and became pregnant of a boy; at the third month the pregnancy, which proved to be tubal, was terminated by the bursting of the tube which had subsequently to be removed. The mother was saved, and it was found that, though the child was a boy, the offending tube was the left one; and apparently since the birth of the last girl this tube had remained abnormally enlarged, and in an unhealthy condition, thus causing this [151]anomaly. Eighteen months later the lady conceived again; she miscarried of another boy, and the right ovary was left in a state of acute irritation and bound down with adhesions. It is some years since this happened, and she has now succeeded in regaining her normal health and has at last produced a much-needed son and heir.
“Placenta prævia” proves the complete vertical journey of the ovum; in such cases, the ovum, having arrived in the womb, drops vertically downwards to the lower part of that organ, instead of becoming embedded in the upper part. Fertilisation ensues and the fœtus becomes attached to the mouth of the womb, and if the child goes full time it is usually born dead. Ovarian pregnancies are equally dangerous though fortunately rare.
Such abnormalities in no way reflect on the truth of the side theory; on the contrary the abundant evidence I have collected corroborates in every particular that the right side is proper to male issue, the left to female.
[152]
Hitherto no theory has been advanced which explained, in any satisfactory or credible manner, the conception of twins of opposite sex. I maintain, however, that, in the light of my investigations, it becomes a simple and natural occurrence, and in this chapter I will briefly outline the circumstances from which it may arise.
Twins may be conceived in two or three different ways:
1. A boy may have started at the beginning of the month, or toward the middle, and a girl may be conceived seven days later or [153]more, just before the next period is due; the fact that the uterus does not always close up entirely, and may even slightly re-open after conception, has been sufficiently proved to make such an event entirely probable. To give an instance, an American biologist mentions the case of a white woman who gave birth to twins on two successive days, of which one was white and the other black. She subsequently admitted intercourse with a coloured man a few days after her husband had left her for a long period. Quite clearly this woman conceived each twin on a different day, by a different father.
The fact that so often, where the twins are of opposite sexes, one seems to be less developed than the other, points to the probability of one of them having been conceived one, two or three weeks later than the other. When the girl is the smaller, which is often the case, we may conclude she was the last conceived. If the boy be the smaller he was conceived perhaps at a later date, and after the attempt [154]at menstruation which often occurs during the first or second month of girl-pregnancy. I believe this manner of twin-conception to be rare, however. Out of twelve cases of mixed twins collected recently, I have found only one where the boy was smaller.
2. A boy may be conceived simultaneously with a girl if the ova from both ovaries happen to be present in the tubes or uterus at the same time. This would occur in the “blank week,” which, as we explained previously, does not exist for certain women, if their period arrives every three weeks. So, at the end of fifteen days, from the first day of period, the left ovary, already active, his discharged an ovum before the male ovum discharged by the right ovary has fully lost its vitality. Where this is the case, both of these ova are equally ready for fertilisation. This manner of conception is probably much rarer than that first considered. It is very unlikely that a woman of irregular habits could produce two ova each capable of forming a healthy embryo.
[155]
3. The conception of mixed twins has been explained in the following way:—It is known that healthy spermatozoa may live for weeks in a woman’s Fallopian tube. Thus, the male ovum having been fertilised on the twelfth day or so after the first day of period, the female ovum may be fertilised by the same issue of spermatozoa some ten days later. This would also account for the smaller weight at birth of the girl. Any exception, where the girl was the finer specimen of the two, might be explained either by the arrested development of the male infant, owing to a less healthy male ovary, or by the cornu of the uterus on that side being less elastic and so preventing as full a development as that on the left side.
This last theory of conception, which has the support of many biologists, does not appear to me to be satisfactory. How can the fertilisation of the left ovum by the belated spermatozoa be really effective? And, if it is so, would not the lack of spontaneous vitality account for those arrested pregnancies one so [156]often comes across, and for which, up to now, no cogent reason has been advanced? Faulty fertilisation might as well be the cause of an abortion at any early state of one embryo whilst the other continues its normal course.
I knew of one woman who, having had a mishap at thirteen weeks of a male fœtus, was surprised on getting up again to find that she was still pregnant. Five months later she gave birth to a healthy girl. Dr. Jameson cites the following case. A lady he attended was delivered on February 13 of a healthy male child, whom she nursed. On April 3, however she was taken ill, and shortly after was confined of a blighted fœtus, between eight and nine inches long. This fœtus was attached to a placenta, which appeared to be quite healthy, as large as that belonging to a full-grown one.[27] Great numbers of such cases may be quoted, but till recently the causes have been obscure.
It is commonly believed that when twins are [157]of mixed sex one or the other proves sterile when adult and there seems some ground for this assumption, but it is not of universal application.
Difficult as it was, I have made every effort to get at the facts, with the result that in scores of cases one or other of the twins has been found to have remained celibate, or, after marriage, to have had no children. I know of three sets only of mixed twins where both have married and had families.
The bearing of twins apparently tends to be hereditary in the female line, often recurring from mother to daughter, and this is more frequently the case where the twins are of the same sex. These are the result of a special development of one ovary or the other, accompanied by a propensity to discharge two ripe ova simultaneously.
Triplets, quadruplets, and quintuplets are likewise produced for similar reasons, as above described. In May, 1915, a Mrs. Howarth of Sheffield gave birth to three boys and one [158]girl. They have all survived and done well. “An Italian woman at Palermo has given birth to five children, all of whom are in perfect health,” was an announcement which appeared in the papers not many months ago.
Such occurrences are quite tame compared to the account given by Ploss of an Italian woman, named Dorothea, who in two births produced twenty sons.[28] First, a bevy of nine arrived, and two years later eleven more boys were born at one birth, these happenings being substantiated and vouched for by the doctors Francesco Pico della Mirandola and Ambrose Paré. The engraving, made from an authentic picture of this woman before the birth of her many sons, is most extraordinary to behold: the curious thing is that all were male children, so evidently the woman had a right ovary abnormally developed to the complete extinction of the left. Statistics go to prove, however, that the birth of female twins [159]is more common than that of male.[29] No doubt this is, in a measure, due to the greater difficulty of carrying male twins.
I knew of a woman who, within two years, gave birth to two sets of male twins; she subsequently bore first a single boy, and then a triplet of boys. Her left ovary had previously been removed, as the result of an unfortunate confinement when a girl-child was still-born; but she did not carry the first male twins longer than a bare thirty-three weeks. Had she carried them to their full term, it is doubtful whether she would have made a normal recovery and been able to produce the other six boys.
Those women always recover most easily from boy twins who do not carry them full time, and whose babies, when born, weigh barely from four to five pounds each. Twins weighing together twelve pounds or more at birth tend to overstrain the genital organs of the mother, with bad results. The tube is [160]frequently left in a disastrously distended condition, which may lead to tubal pregnancies and appendix trouble.
Girl twins are seldom carried over eight months and are usually small, entailing infinitely less strain on the mother. They are not only more frequent, but easier to rear than boy twins. Mixed twins are the most usual of any, and they are rarely like each other, whether in looks or character. If they are very large, the result to the mother may subsequently be sterility, but this is not by any means to be taken as a general rule. I have known a woman start a fine family of six sons and six daughters with a good-sized set of mixed twins.
Mr. Rumley Dawson divides twins into four varieties:
Variety A. One Boy: One Girl: One from each ovary—a different Graafian follicle: a different ovum: generally one placenta to each.
Variety B. Two of the same sex: One ovary: two Graafian follicles: two ova: either [161]two girls or two boys. In this variety there may or may not be a placenta to each, but generally there is only one.
Variety C. One Sex: one ovary: two ova contained in the same Graafian follicle. One corpus luteum only will ensue from the bursting of this Graafian follicle which contains two ovuli. In this case the children will resemble each other—far more closely than those coming under the first two categories. One placenta only will be found.
Variety D. One Sex: one ovary: one Graafian follicle and one ovum in which are contained two nuclei. These twins are rare, once in seven only. Extremely similar they are often joined together like the “Siamese Twins.” In triplets the same conditions obtain, and one ovum may produce three nuclei, all of the same sex.
As I have shown, twins are conceived according to all the rules laid down by the much-discussed, but hitherto imperfectly, understood, [162]side-theory, and, where it was well-nigh impossible to explain clearly the conception of twins of mixed sex, complete understanding is now afforded by our newly acquired knowledge of the functioning of the left ovary.
That twins are the result of a peculiar condition of the ovary, usually hereditary, I have already indicated; it clearly follows therefore that multiple pregnancy cannot be initiated at the parental wish. But, where there is a marked family inclination to twins, it is certainly possible to ensure their being male or female, according to desire, provided they be both of the same sex.
[163]
Hippocrates maintained that the male fœtus became animated thirty days after conception, while the female required forty-two days to become animate. This exactly bears out, and is explained by, the theory set out in my formula that a male conception occurs during certain days after the period, and a female somewhere between the twenty-first and twenty-eighth day: that is, eight to twelve days later.
Montgomery, in the year 1850, was of the opinion that conception could occur apart from the previous influence of menstruation. For, as he said, if they are necessarily dependent the one on the other, “no woman could conceive [164]at any time, except at, or just after, the menstrual period.” And in support of this he refers to instances of women who, having never menstruated, yet became pregnant, and also of girls who had borne children before they menstruated.[30]
In such an event the left ovary would always be the first to operate. Nysten records the case of a girl of thirteen, who, having not yet menstruated, died at the Hotel Dieu, Paris; after death a tumour was found in the situation of her left ovary, having every appearance of a blighted fœtus.[31] In my investigations I observed the case of a village girl of nineteen who became pregnant, and at seven months was taken seriously ill. Up to the actual moment of parturition, both the midwife and the girl’s mother refused to believe that the labour pains could betoken a possible pregnancy, as the patient had never menstruated; she gave birth to a premature female infant.
[165]
A young married woman, whom I met recently, gave birth to a baby girl, although she had not menstruated for two years before becoming pregnant, and could give no dates to her doctor for calculating the date of the babe’s arrival.
Mr. Whitehead, of Manchester, has given particulars of nine cases in which pregnancy occurred previous to menstruation. He did not give the sex of the offspring, but, according to all the evidence I have been able to collect, such pregnancies almost invariably result in female issue.
My explanation is that menstruation was either temporarily suppressed, or that it did occur, but was so scanty as hardly to be recognised for a normal period. We must, therefore, accept it as extremely unlikely that ovulation which, as before explained, is the discharge of a ripe ovum, can occur apart from the influence of menstruation.
Biologists, who at one time believed that ovulation must happen simultaneously with [166]menstruation, found it difficult to account for the large numbers of conceptions occurring before the beginning of the catamenial flow, or after its complete cessation. The suggestion that the spermatozoa might lie in wait for the ovum is not reasonable, taking into consideration that the actual monthly discharge, when at its height, would almost certainly carry off the spermatozoon, which is still in the nature of a foreign body until it has fertilised the ovum.
Another popular idea is that ovulation and fertilisation are spontaneous. This implies a necessary state of consciousness and active responsiveness on the part of the female, which cannot be backed by any kind of circumstantial evidence. Too many examples exist of women who not only had no sensation during conception, but became pregnant under the influence of drugs, asphyxia, drunkenness or even deep sleep. Also the fact of rape, which has so often resulted in offspring, again disposes of the natural and perhaps more pleasant [167]conclusion of mutual spontaneity in impregnation. It must strike one that nature seems to have made a slip in this respect, thereby involving in undue horrors and anxiety the victim of criminal assault.
According to Montgomery, a woman may be delivered during sleep, without being conscious even of first labour. This must be of rare occurrence, especially among women who have not previously borne children and whose organs are thus less disposed to dilate; it might be possible in warmer countries than those of Europe. A lady told me her first three children, born in India, gave her no trouble at all, but during her last three confinements in England she nearly lost her life each time; and it is well known that most Anglo-Indians prefer an Indian confinement to a home one. There is no doubt that the summer confinement is, as a rule, quicker and easier for the same patient than one occurring in winter.
But this is a digression. To return to my [168]argument, there exists no biological fact to dispute the theory that the ovum, whether before or after the menstrual period, may lie for a few days awaiting fertilisation. It is entirely unreasonable to suppose that the catamenial flow might carry away, not only all belated spermatozoa, but even the ovum itself. So for that very reason, the ovum is discharged separately from the flow, although in direct relation to it. Thus, one month it is thrown out after the uterus has been emptied of its menstrual flow, and the next month it is thrown out before the period is due, and some seven or eight days previous to the actual discharge. This is the normal rule. The exception occurs when an abnormal ovary allows the ovum to escape during the period; even then it happens only after the bulk of the discharge has been eliminated from the ovary. Thus nature protects the ovum, which otherwise might well be carried away by the purifying process of the period at its height.
With reference to menstruation occurring [169]during pregnancy, Montgomery says: “The safety of the ovum would appear incompatible with the profuse and frequently repeated discharge which some women experience, without abortion ensuing.” At the same time there appears to be no reason, anatomical or physiological, why a certain amount of menstrual discharge should not escape in the ordinary way, but, should it do so, it is bound to interfere with the well-being of the ovum.
A woman I knew had a fine boy whom she nursed, although menstruation started at the second month, and continued regularly. But her horror was great when she noticed that her figure was growing in size, and when the “quickening” at four months assured her that she was again pregnant, she weaned her boy at once; but the menses continued until she gave birth to a puny six-month boy, still-born as the result of this triple strain on the maternal constitution.
It is the apparently independent action of ovulation and menstruation which has so often [170]puzzled biologists of all ages, affording, as it does, ample explanation of the doubts they have expressed as to the possibility of any allied action between them. Menstruation without ovulation may possibly take place, but can ovulation happen without menstruation? The presence in the ovary of the ripening Graafian follicle doubtless encourages the catamenial flow to start, in the one case before its actual rupture, and in the other seven days after it has burst and thrown out the ovum into the tube, but the menses may occur equally where ovulation is immature, faulty or entirely absent.
However this may be, it must be insisted on that conception during the actual flow cannot take place, for the reason that the embryo, in all probability, would be carried off with the bulk of the natural discharge. But after the second or third day this is usually scanty and slow, insufficient to disturb a possible fertilisation. Such happenings, however, are not desirable. However scant the discharge or even [171]if it be quite dried up, the uterus should in no wise be disturbed before the eighth day.
Even so, where a “freak” ovary is suspected, should intercourse happen in the fruitless month, it is desirable to take a hot douche for three successive days after the seventh day of period. This clears away danger of conception from a “freak” ovary. Such a practice, further, is not only entirely harmless, but cleanly and productive of much local comfort and well-being. Where there is danger of undesirable fertilisation, it is the one and only decent means of avoiding such an occurrence; otherwise the alternative is to resort to “birth control” methods of a less healthy or desirable nature. Even in the fruitful month, healthy conception is not desirable before the eighth or ninth day of period, i.e. two or three days after the cessation of the actual flow.
Throughout this book I have endeavoured to make clear how it is possible to avoid such pitfalls. By adhering to the times and dates set forth in the preceding chapters, every [172]healthy and regular woman can ensure the normal conception and pregnancy of a child, boy or girl as she desires. Not only is she assured of immunity from the advent of undesired offspring, but also the power is placed in her hands of limiting the number of her children, without having recourse to methods prejudicial alike to the sources of health and happiness.
[173]
It has frequently been asked in the course of discussions on the alternate action of the ovaries, whether both take an active part in each pregnancy. We have seen that after the removal of one ovary, the other, in due course, takes to itself the work of both, doing double duty and thus allowing menstruation to proceed on more or less normal lines. Similarly it may be concluded that, supposing the right ovary has produced a fertile ovum, the left one will remain inactive during the whole period of pregnancy, ceasing both to ovulate and to menstruate. Thus, the entire alimentary [174]discharge is left for the use of the right ovary, which by sole reason of its activity attracts and distributes the double supply. Moreover, the placenta is supplied direct from this ovary with sanguine nutrition wherewith to feed the fœtus, and it is interesting to note that Jaquemier specified anæmia in numbers of women as commencing after the middle period of pregnancy; this is accounted for by the huge supply of blood nutriment absorbed by the placenta feeding the fœtus.
Another theory, however, is that ovulation and menstruation of both ovaries do continue during gestation, but that the one ovary does not directly feed the ovum of its rival, but passes its alimentary fluid to the opposite side—by so doing directly helping to sustain the fœtus. But all evidence I have collected seems to point to the former theory. No doubt, in the case of mixed twins, both ovaries concur directly and alternatively in the nourishment of their own fertilised ova.
In post-mortems on women advanced in [175]pregnancy, the corpus luteum has been found in the ovary whence came the embryo, according to its sex. While on the opposite side no fresh scars of false corpura lutea from recent menstruation were found, although within a few weeks these would certainly have shown a distinct yellow mark on the ovarian surface; from this we gather that the last false corpus luteum formed in that ovary appeared before the commencement of the pregnancy.
Another point that should be made quite clear is that relating to the duration of gestation, which differs according to the sex of the child. Dr. Chavasse was of the opinion that, as girls so often seemed to arrive at the beginning of the month as counted from the last period, they were evidently conceived after the period, whereas boys, he argued, arriving often at the end of the month and generally later than was expected, were evidently conceived at the end of the month and a few modern physicians still uphold this theory. But, needless to say, it is entirely erroneous. Chavasse [176]says also he is inclined to believe that girls are carried longer than boys. This, again, is exactly the reverse of the facts, if we study them in a clear light, considering them as they actually are and not as they appear to be.
A boy takes longer to mature in the uterus than a female for two reasons:
1. He does not, as previously explained, find the preparation of decidua in the uterus; hence a slower development in the early stages.
2. He weighs at birth about 1 lb. more than the average girl; so he requires extra time in which to develop.
French medical authorities cherish the idea of longer girl-gestation for the reason that a female fœtus will, they say, often be carried fully thirty-nine weeks and she may even, though this is rare, be carried forty weeks, but when this happens in the case of a girl, the pregnancy becomes “protracted,” and the result is either an enormous child, weighing from 11 to 12 lbs., or an arrested and abnormal pregnancy. A boy usually goes his full thirty-nine [177]weeks; often he is carried forty, or even sometimes forty-one weeks; thus, though begun after the period, he will yet run right on to the end of the ninth month, or into the tenth month of gestation.
Personally I have rarely met with the case of a girl-child of under 7 lbs. weight, carried beyond thirty-eight weeks; thirty-nine is the extreme normal limit, and results in a child weighing from 7-8 lbs. at least; forty weeks is abnormal. I know many families of girls where each was carried barely thirty-six or thirty-seven weeks; they were all healthy and normal, weighing from 5-7 lbs. It may be that the greater restlessness of the female fœtus hurries, to some extent, the process of girl-gestation; and the fact that anæmia is very frequent during girl-pregnancies may be the cause of less endurance in the mother, and helps to explain why girl-babies are carried a shorter time. It is never safe to count on a nine-month gestation with a girl. Real “full-time” girl-babies are exceptions to the rule, [178]and often a mistake arises through the belief that a child was conceived two or three weeks previous to its real date of conception. Frequently mothers show me new-born babies weighing 4½ to 5 lbs., with the remark, “Yes, I carried her full-time; it was close on nine months since my last period when she was born,” and in nine cases out of ten these infants have been carried barely thirty-six weeks. Yet they grow and flourish as well as the “full-time” babies.
Anyone who has been in a position to await and watch, as I have, great numbers of births, cannot fail to have noticed that the girl baby comes unexpectedly early, often before preparations have been completed.
The boy, on the contrary, looked for daily, withholds his advent, often from week to week; and this must be recognised as the normal distinction.
Nature works slowly and discreetly; she is chary of revealing her secrets, and few of [179]those, eager for practical results, could have afforded the life-time of work, which I have been able to give, for the continuous investigation that was necessary.
As regards my personal experience and the results obtained I can but say that they have uniformly realised my highest expectations. In every case where my formula was employed, there has been success, and I can point to thousands of accurate results. The theory, as a whole, has worked out consistently all the time, and in the few cases where a disappointment has occurred it has invariably been proved to the hilt that the formula was not accurately followed.
I recall the case of a lady who had my formula for a boy; she wrote to me in October, 1913:
I came across a doctor who holds opposite theories to ours, i.e., first ten days a girl, last ten days a boy, based on his practice, which is pretty large. I was disappointed to find anyone whose experience worked out contrary to yours. I am by [180]way of having an infant in December, having followed out your theory. So we shall have to wait and see results, but I feel rather disappointed....
Result—a boy born December, 1913.
This is one of many similar epistles, but in each case the issue has been as arranged for. It is curious to note here that, apart from accidents, a child is born on the actual day of the week that it was conceived; and this detail might well be made use of with reference to the future day of its birth.
This book may come as a shock to some biologists, especially those who have been unable to give to these matters the close practical observation necessary for solving such a problem as that with which it deals. It may appear to them outrageous that a mere woman should write so openly, putting the choice of her children’s sex within the reach of every mother, and, without compunction or hesitation, expounding these secret laws of nature for the benefit of humanity.
[181]
It is, however, unlikely that any male practitioner would have found the time, even supposing he had the mind and the opportunities to follow up this exclusive study of one subject in all its minor details and side-issues. It is only a woman who could possibly have made the unique series of observations that I have found absolutely necessary in the pursuit of knowledge so long denied to parenthood. Could any but a woman have ferreted out the exact dates and times of conception in scores of pregnancy cases, or follow minutely every detail and symptom, week by week, month by month, up to the time of parturition?
The very simplicity of my formula, which in no way disturbs the course of nature’s laws, has often provoked the comment, “Surely it’s all too simple to be true. Why was it never found out before?” In reply I would remind my readers of Christopher Columbus and his egg! And is there not a saying, “The greatest truths are the simplest?”
My final word is this: Time will prove, more [182]and more abundantly, that the knowledge disclosed to us by nature’s teaching deeply concerns the whole scheme of life, and must have its effect on the welfare of the human race.
There may be—there is—more to learn and to discover. I do not assume complete knowledge of every contingent problem, but what I set out to do has been accomplished in so far that every woman can, with certainty, claim complete mastery in the regulation of the sex of her offspring.
[183]
When widespread attention was called in the Press, some months before the publication of this book, to the nature of my discovery and the theory I have based on it, there were not wanting one or two critics who thought fit mildly to question it, doing so, incidentally, with only very partial knowledge.
By far the best answer to such criticisms is the fact of the practical success of my theory as demonstrated by actual results. Extracts from a few of the great number of letters received, which were naturally of a private and confidential nature, are here set forth and these could be multiplied indefinitely. Nothing could, to my mind, be more distasteful than anything savouring in the slightest degree of advertisement, but I feel bound to use what is [184]the most effective of all methods in bringing home to enquirers proof of the success which has attended the application of my theory. I should add that all the letters received were purely spontaneous expressions of gratitude:
“I had a small son born last September. I was most delighted with his sex ... after two little girls, and I wish to thank you for your assistance and advice.” (1914)
“It all happened exactly as you said, every date was correct, my boy weighed 10 lbs. at birth; thanking you again for all your kind help.” (1913)
“You will be sorry to hear that I had a miscarriage.... But it was a boy according to your theory—thus proving that your advice was correct.” (1915)
“I must tell you that my wife had a boy on the afternoon of the 1st. She desires me to write and thank you for your advice.” (1915)
“Our wee boy arrived two weeks ago—yet another triumph for you. I cannot tell you how thankful I am for all your good advice.” (1916)
[185]
“It is splendid having this baby-boy after four girls; it has changed our whole life.... A thousand thanks.” (1920)
“It was kind of you to provide Mrs. C. with a son! There were great rejoicings, after three daughters.” (1912)
“I followed out the instructions and the results are magnificent.” (1914)
“I followed your directions and started a child ... it was a boy, proving your theory correct: eighteen months later, again following your instructions, I had another boy.” (1915)
“I am forty-one, my two girls are twelve and ten. Since the doctor said I could have another child, I have unfortunately had no result; I should not think of another if it was going to be a daughter, but I should love a son.” (1918)
(A year later.) “We are all so delighted at having a son and think you need our grateful thanks.”
“I write as soon as I can to say how immensely grateful I am to you for the son I have been wanting for the last seven years. He is called —— after my father. Both my brothers were killed in the war, so I did very specially want a boy, and now [186]I hope to have more owing to you. I think your discovery one of the most important that can be made, and only long for everyone to know of it.” (1925. Received while the proofs of this work are passing through the press.)
“I wrote to you for a daughter a year ago.... A very precious little girl arrived in November. I am more grateful than I can say.” (1912)
From South Africa.
“Thank you for your letter. It may interest you to know that my three boys started on the day you give for conception of males, and I am positive the little girl I lost started a week before the period. Thank you so much for your advice. I hope my new baby-girl will have arrived next time I write.” (1922)
(A year later.) “Just to let you know our lovely baby-girl arrived a month ago.”
“I am so delighted with my daughter and was so well all the time. I feel so full of gratitude.” (1919)
“My friend, Mrs. P., has her baby girl according to your hints, and she is very grateful to you.” (1923)
[187]
“It was an amazement to me when I found I had started, as all the specialists told me I could not possibly have another child. I had an easy confinement; the boy weighed 9½ lbs. Many, many thanks. I intend giving your address to many mothers who need your recipe.” (1917)
“I find it hard to express how awfully grateful I am to you for all you have done.... It really is too extraordinary what you have done for my health, besides the infant—your power is so wonderful, and the happiness you bring to people.” (1913)
“I cannot half express my gratitude to you. It seems just like a miracle ... I am deeply grateful....” (1916)
“I can’t tell you what a joy our little girl is to us. I never can be grateful enough. Do help my friend as you helped me.” (1924. This lady had been childless for fifteen years.)
[1] Pure Sociology, p. 313.
[2] L. Schenk: Determination of Sex.
[3] R. C. Punnett: Mendelism.
[4] Tennessee Lady Cook: Essays.
[5] In the mishaps that I have observed, the first bad sign is very frequently the total disappearance of all kinds of nausea. Montgomery remarks: “There is little doubt that, in general, vomiting is a useful concomitant in pregnancy, and that its sudden cessation is very often indicative of an unfavorable change in the contents of the womb, and of approaching abortion.”
[6] Psychotherapy, p. 19.
[7] Lancet, April 23, 1842, p. 119.
[8] Speech by Mr. Wheatley (Minister of Health, 1924) to the Standing Joint Committee of the Independent Women’s Organisation, July 31, 1924.
[9] Advice to a Wife.
[10] Sterility of Woman, 1890.
[11] Edinburgh Medical and Surgical Journal, vol. 38, p. 231.
[12] Médecine Légale.
[13] Traité des accouchements, obs. xxiii, p. 52.
[14] Medical Jurisprudence, vol. i, p. 257.
[15] Transylvania Medical Journal, vol. vii, p. 447.
[16] Sex Causation.
[17] Address to the British Association, 11th Aug., 1924.
[18] Leviticus xv, 24.
[19] On the Nature of the Child. Section 11.
[20] Pract. Obs., p. 107.
[21] Introduction to Midwifery, 5th Edition, p. 217.
[22] Leviticus xx, 18.
[23] Leviticus xii, 2.
[24] Brit. and For. Med. Rev., Oct., 1842, p. 386.
[25] Robertson: Essays, p. 92.
[26] Verhanlungen der Phys. Med. Gesellschaft in Würzburg, Bid. iv, 1853.
[27] Dub. Med. Journ., vol. xxii, p. 15.
[28] Das Weib, p. 787.
[29] Playfair: Science and Practice of Midwifery.
[30] Montgomery: Signs and Symptoms of Pregnancy.
[31] Convisart et Leroux: Journal de Médecine.